



INTRODUCTION
Wide-necked intracranial aneurysms are a challenge for endovascular treatment due to its risk of coil protrusion in the parent artery and aneurysm recurrence. In 2002, the first specific stent to assist in the coiling of wide necked aneurysms was introduced [3]. Since then, stent-assisted coiling has been established as a treatment option for these challenging aneurysms, as the stent provides a mechanical scaffold to prevent coil protrusion. Furthermore, the hemodynamic and biological effects of stents promote progressive aneurysm thrombosis and impede recanalization [21,23]. However, despite the significant contributions of stents, the endovascular treatment of complex bifurcation aneurysms with a multibranch neck still remains a challenge for surgeons. Several reports have indicated that Y-configuration stent-assisted coiling provides improved durability [14,18,26] and facilitates coil embolization in situations untreatable with conventional stents alone [24,25].
Since Chow et al.’s first report on Y-stent-assisted coiling [12], several types of early neurovascular Y-stents have been reported, all delivered through microcatheters with an internal diameter of 0.027 or 0.021-inch [6,12,14,26]. However, due to their relatively large profiles, these catheters are often difficult to navigate through the sharply angled side branches of bifurcations. Furthermore, during Y-stenting, attempts to perform catheterization with these relatively large profile catheters through the struts of the initially deployed stent might result in stent deformation and dislocation [1,6].
Recently, new low-profile stents have been introduced for the treatment of wide-necked aneurysms. Among them, the Neuroform Atlas stent (Stryker Neurovascular, Kalamazoo, MI, USA), a microcatheter-delivered, self-expanding, mixed open-cell/closed-cell stent, has been widely used. Compatible with a 0.0165-inch microcatheter, it allows easier navigation through small-sized, delicate vessels and, thereby, improves the safety of stenting during distal wide-necked aneurysm treatment [2,4,10]. The deliverability through low-profile microcatheters and its open-cell design are the technical features that allow a safe Y-stenting procedure. A recent case series assessing the outcomes of stent-assisted coiling procedures using Neuroform Atlas stents provided promising results [10,16,17,28]. However, the number of reports on cases treated with Y-stent-assisted coiling and Neuroform Atlas stents is very limited [5,9,13,16,28]. In this retrospective study, we aim to report our findings on Neuroform Atlas Y-stenting for coiling of wide-neck aneurysms at various bifurcation locations.
MATERIALS AND METHODS
Patient selection
This retrospective study was approved by our Institutional Review Board, who waived the requirement for informed consent. The Neuroform Atlas was approved for use in our country in March 2018. From March 2018 to January 2021, we treated 473 aneurysms in 436 patients with coil embolization. We retrospectively reviewed the characteristics of the patients and the aneurysms, procedure-related complications, radiographic results, and clinical outcomes. There were 15 cases of wide-necked bifurcation aneurysms (all unruptured) treated by Y-stent-assisted coiling and two Neuroform Atlas stents. All 15 cases underwent digital subtraction angiography (DSA) and rotational angiography with three-dimensional (3D) reconstructions to characterize the anatomy of the aneurysm and parent artery. Widenecked aneurysms were defined as aneurysms with a dome-to-neck ratio <2 or a neck diameter >4 mm. Complex bifurcation aneurysms were defined as wide-necked bifurcation aneurysms that incorporated >1 side branch of the bifurcation.
Dual antiplatelet medication (aspirin 100 mg and clopidogrel 75 mg) was administered for ≥5-7 days before treatment. Platelet function testing was routinely performed for all patients. After the procedure, patients were prescribed 75 mg of clopidogrel daily for 3 months and 100 mg of aspirin daily for ≥12 months. Routine clinical follow-up was conducted at around 1, 3, 6, 12 and 24 months based on our hospital’s protocol. Vascular imaging follow-up was performed with magnetic resonance angiography (MRA) or DSA.
Neuroform Atlas Y-stent coiling
All procedures were conducted under general anesthesia. A 5-Fr to 7-Fr guiding catheter was positioned in the internal carotid artery (ICA) for anterior circulation aneurysms, and a 5-Fr or 6-Fr guiding catheter in the vertebral artery for posterior circulation aneurysms. Intravenous systemic heparin (50 U/kg) was administered while placing the guiding catheter. An activated clotting time of 2-2.5 times that of baseline was maintained during endovascular treatment. The first Excelsior SL-10 microcatheter (Stryker Neurovascular) was introduced and advanced over a 0.014-inch guidewire into one branch of the parent artery. The aneurysm sac was selected with the second Excelsior SL-10 microcatheter, and the first Neuroform Atlas stent (Stryker Neurovascular) deployed across the aneurysm neck, with jailing of the preplaced first microcatheter within the aneurysm sac. The first microcatheter was re-advanced over the stent-loaded delivery wire within the first stent up to the aneurysm neck, and the stent-loaded delivery wire removed. The other branch was navigated through the first stent struts using a 0.014-inch microwire, followed by advance of the first microcatheter over the wire. The second Neuroform Atlas stent was deployed in a Y-configuration, and coiling was performed using the second microcatheter with its tip within the aneurysm sac and jailed by two Neuroform Atlas stents in a Y-configuration.
Outcome measurement
Procedural success was defined as the full expansion of two Neuroform Atlas stents in a Y-configuration, except at the through-struts crossing point of the second stent and complete coverage of the aneurysm neck. Angiographic results and clinical outcomes were reviewed retrospectively. Clinical and angiographic follow-up between 1 and 28 months (mean, 12.3 months) after the procedure was performed in all patients. The clinical outcomes were assessed by Glasgow Outcome Score (GOS) score at the time of discharge and the latest clinical follow-up. Treatment-related morbidity was defined as development of any new neurological deficit due to treatment-related complications still present at discharge. Treatment-related mortality was defined as death from treatment-related complications during admission or clinical follow-up. The angiographic results were evaluated by two independent investigators and categorized as complete occlusion (without a neck remnant), neck remnant (>90% occlusion with small neck remnant or dog ear), or incomplete occlusion (filling of the aneurysm lumen). Follow-up imaging outcomes were also classified as (1) improved or stable aneurysm occlusion, (2) minor recurrence not requiring re-treatment, and (3) major recurrence requiring re-treatment.
RESULTS
Neuroform Atlas Y-stenting was successfully attempted in 15 patients with 15 unruptured wide-neck bifurcation aneurysms. The patient group comprised 6 men and 9 women with a mean age ± standard deviation of 56.4±6.6 years. The aneurysm was located in the anterior communicating artery top in eight, middle cerebral artery (MCA) bifurcation in three, basilar artery bifurcation in three, and ICA bifurcation in one patient. The mean dome and neck sizes were 6.4±3.1 mm and 4.7±1.8 mm, respectively. Neuroform Atlas Y-stent-assisted coiling was planned as initial treatment in nine patients and as salvage treatment in six patients. Among the latter, four cases were due to coil protrusion, one to coil migration, and another to thrombosis. Immediate post-procedural angiograms showed complete occlusion in 46.7% of cases, neck remnant in 13.3%, and incomplete occlusion in 40%. No treatment-related morbidity or mortality was described in any patients, except for a transient ischemic attack with caudate head infarction, but no permanent morbidity. All 15 patients had good clinical outcomes, as shown by a GOS score=5 at both discharge and at a mean of 12.3-month (range 1-28 months) follow-up. Further, all aneurysms showed improved or stable aneurysm occlusion on follow-up imaging. Particularly, follow-up angiography showed complete occlusion in 73.3%, neck remnant in 6.7%, and incomplete occlusion in 20% of cases. Clinical and angiographic data are summarized in Table 1.
Case illustration
Case 2
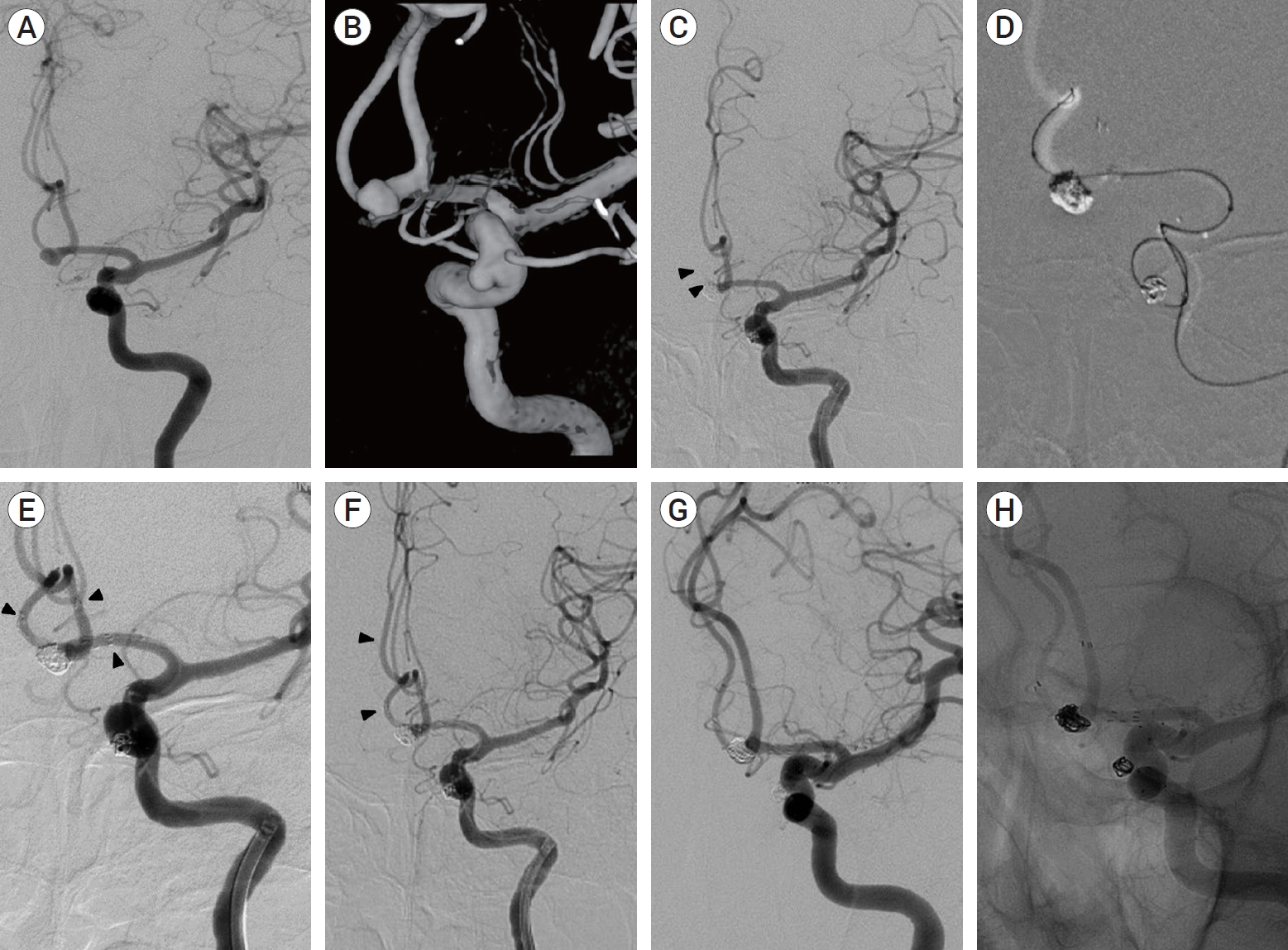
A 69-year-old woman with no previous history presented with incidental findings of anterior communicating artery aneurysm and left superior hypophyseal artery aneurysm diagnosed on computed tomography angiogram. Cerebral angiography revealed a relatively wide-necked saccular anterior communicating artery aneurysm approximately 5.72 mm in maximal length, with a neck length of 3.81 mm, and 3.48 mm in height; the wide-necked left superior hypophyseal artery aneurysm was approximately 3.44 mm in maximal length, with a neck length of 4.02 mm, and 3.02 mm in height (Fig. 1A, B). Both aneurysms were treated in a single endovascular treatment. A 6 Fr-guiding catheter was placed in the left ICA. The first microcatheter (Excelsior SL-10 “90 degrees”) was navigated into the left A1 through the A2. The aneurysm was selected by the second microcatheter (Excelsior SL-10 “straight”). We deployed a Neuroform Atlas stent (3.0 mm×15 mm) in the left A2 to left A1, and a total of four coils were inserted into the aneurysmal sac. Immediate follow-up angiography showed near complete aneurysm occlusion and intact parent artery flow. We performed another stent-assisted coiling technique for the left superior hypophyseal artery aneurysm with a Neuroform Atlas stent (4.5 mm×15 mm). However, final angiography revealed flow delay in the right anterior cerebral artery due to thrombosis and compensated by collateral flow (Fig. 1C). A microcatheter (Excelsior SL-10 “S”) was navigated into the right A1 through previous stents via the cell-through technique (Fig. 1D). Tirofiban (0.75 mg) was injected, and another Neuroform Atlas stent was (3.0 mm×15 mm) deployed from the right A2 to left A1, achieving salvage Y-stenting (Fig. 1E). Immediate and delayed 10-minute post-procedural angiography revealed intact flow in both anterior cerebral arteries (Fig. 1F). The patient was discharged without any complication or neurologic deficit. Both the 12-month follow-up angiography and 24-month follow-up MRA showed complete occlusion in both aneurysms (Fig. 1G, H). Further, the patient presented no symptoms throughout the follow-up period.
Case 12
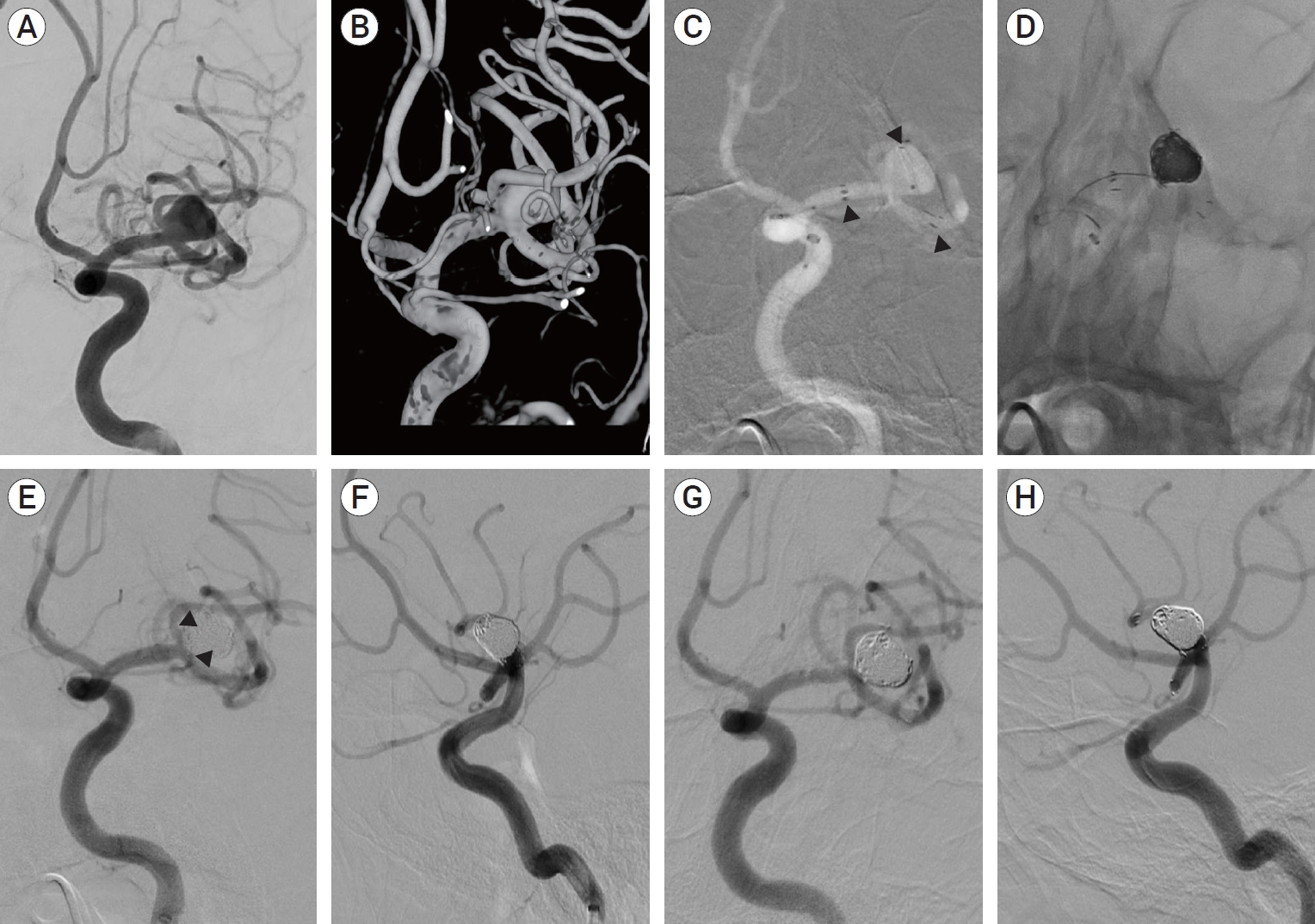
A 58-year-old woman with a history of hypertension and dyslipidemia presented with an incidental finding of left MCA bifurcation aneurysm diagnosed on MRA. Cerebral angiography revealed an aneurysm approximately 9.30 mm in maximal length, of 5.69 mm neck length, and 6.47 mm in height (Fig. 2A, B). During endovascular treatment, a 6 Fr-guiding catheter was placed in the carotid siphon of the left ICA. The first microcatheter (pre-shaped Excelsior SL-10) was steam-shaped into a “J” and navigated into the superior division of the left M2. The aneurysm was selected by the second microcatheter (Excelsior SL-10 “straight”), and a Neuroform Atlas stent (3.0 mm×15 mm) was deployed in the left M1 to the superior M2 division. The first microcatheter was moved into the inferior division of the left M2 via a cell-through technique. Then, the second Neuroform Atlas stent (3.0 mm×15 mm) was placed in the left M1 to the inferior M2 division, achieving Y-stenting (Fig. 2C). A total of six coils were deployed into the aneurysmal sac (Fig. 2D), and initial angiography showed a minimal neck remnant (Fig. 2E, F). The patient was discharged without significant complication or neurologic deficit. However, 3 months after discharge, the patient showed symptoms of transient ischemic attack with right side weakness and dysarthria, and magnetic resonance imaging showed a mild infarct of the left caudate nucleus head. The patient reinitiated dual antiplatelet medication, and afterward, there were no symptoms of neurologic deterioration. The 4-month follow-up MRA and angiography showed complete aneurysm occlusion without any in-stent stenosis and intact patency of the parent arteries (Fig. 2G, H).
DISCUSSION
Complex bifurcation aneurysms have always been a challenge for endovascular surgeons. Due to their wide-necks incorporating >1 branch of the parent artery, conventional stent-assisted coiling alone may not provide good safety and durability outcomes, with high rates of complications such as thrombosis in branching artery or coil migration and protrusion. Various techniques have been introduced for wide-necked bifurcation aneurysms, including horizontal stenting [7], waffle cone configuration stenting [15], and X-configuration [22] or Y-configuration [12] double stenting. Among them, double stent-assisted coiling techniques, including Y-stenting, are an eligible endovascular method for the treatment of complex bifurcation aneurysms.
Despite the potential of Y-stenting for embolization of complex bifurcation aneurysms, it requires several sequential endovascular maneuvers for successful execution. The first challenging part of Y-stent coiling is catheterization and navigation into the sharply angulated side branches. Early neurovascular Y-stents were delivered through microcatheters with an internal diameter of 0.027 or 0.021-inch [6,12,14,26]. Because of their relatively large profiles, these catheters are often difficult to navigate through the sharply angled side branches of bifurcations, leading to lower technical success rates [6]. Recent low-profile stents allow for easier catheterization and navigation in small-sized, delicate vessels and enable safer stent deployment during the embolization of complex bifurcation aneurysms. The Neuroform Atlas stent is one such and can be deployed through low-profile microcatheters, which probably contributed to the low rates of procedural complication in our study.
The second challenging part of Y-stent coiling is the catheterization of the second side branch [6]. Attempts to perform catheterization through the stent struts may result in dislocation of the first stent [1,6,13]. In our cases, however, we experienced no particular technical difficulties during catheterization of the second branch or deployment of the second stents. This may be due to the unique characteristics of the Neuroform Atlas, which is a laser-cut stent with a hybrid cell design combining open and closed cells: the middle part has an open-cell design, while the proximal end has a closed-cell structure [29]. We consider possible that this mixed design facilitated catheterization maneuvers in all our cases. Although several studies reported the safety and efficacy of Y-stenting with closed-cell and braided stents, the closed-cell design of the first stent may cause undesirable synching of the second because of its constrained interstices [19,27].
In general, the immediate aneurysm occlusion rate of Y-stenting is favorable. Limbucci et al. [19] reported an immediate occlusion rate of 87.5% in patients treated with Y-stent-assisted coiling with two closed-cell stents. A recent meta-analysis that investigated the angiographic outcomes of Y-stent-assisted coiling reported an immediate occlusion rate of 82.2%. In our study, the immediate aneurysm occlusion rate was 46.7%, relatively lower than previous Y-stenting studies. However, in our series, 50.0% of partially coiled aneurysms showed progression to thrombosis and a total of 73.3% cases achieved complete occlusion during a mean follow-up of 12.3 months. The elevated occlusion rate during follow-up in our study is compatible with those reported in previous studies [13]. In a meta-analysis that investigated the outcomes of Y-stent-assisted coiling, Cagnazzo et al. [8] found a long-term complete or near complete aneurysm occlusion rate of 95.4%. In conclusion, the long-term follow-up occlusion rate in our study shows that Neuroform Atlas Y-stenting is an effective method for the treatment of complex bifurcation aneurysms.
We attributed the favorable outcomes in long term occlusion rate, despite the relatively low immediate occlusion rate, to specific characteristics of double Y-stenting [11]. Lopes and Sani described complete endothelialization of a Neuroform stent 4 months after its placement in an explanted human aneurysm, with significant de novo fibroelastic tissue formation along the aneurysm neck [20]. The proliferation of endothelial tissue over the stented aneurysmal neck segment can alter the aneurysm’s flow dynamic, promoting thrombosis and stasis inside it. Thus, remodeling the angio-architecture leads to endovascular reconstruction and elicits complete aneurysm occlusion over time. Y-stenting provides excellent intra-aneurysmal flow remodeling through double stents across the aneurysm.
No complication or any definite morbidity was described in our cases. Aydin et al. [5] also reported a low rate of clinical complications (6.7%), and 3.3% permanent morbidity in Neuroform Atlas Y-stenting. This considerably lower complication and morbidity rate differs from previous Y-stent assisted coiling studies [26]. As described earlier, the low profile and mixed opencell design of the Neuroform Atlas stent seems to enable easier access to sharp-angled branches and sufficient expansion of the second stent at the intersection point, leading to high success and lower complication rates. In conclusion, the Neuroform Atlas stent combines the advantages of low-profile deployment microcatheters with an open-cell structure to achieve a safe and successful Y-stenting procedure.
It is noteworthy that in our study the cases where Neuroform Atlas Y-stenting was used as salvage treatment had as much favorable outcome as those with initial Y-stenting. The long-term complete occlusion rate for the salvage treatment was 83.3%, and all 6 patients had a favorable outcome (GOS score=5), maintained throughout follow-up. This result implies that Neuroform Atlas Y-stenting can be a promising salvage treatment if conventional stent-assisted coiling fails due to complications such as thrombosis, coil protrusion, or coil migration.
Due to the inherent limitations of a retrospective study, the effects of possible selection bias cannot be excluded. Further, there was no control group of patients who underwent alternative endovascular treatments. However, in all cases, the endovascular treatment strategy was determined after discussion among vascular neurosurgeons and interventional neuroradiologists. Therefore, selection bias by the primary operator might have had low impact on the results. Another limitation is the relatively small size of the case series and short-term follow-up. A further study in larger populations with complex bifurcation aneurysms is needed to assess long-term safety and durability.
CONCLUSIONS
Y-stent-assisted coiling with Neuroform Atlas stents are a feasible and safe option for wide-necked bifurcation aneurysms. All aneurysms treated with Neuroform Atlas Y-stent-assisted coiling showed improved or stable occlusion during follow-up without any complications or morbidity. Moreover, Neuroform Atlas Y-stents might be a promising salvage treatment after conventional stent-assisted coiling failure.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






