



INTRODUCTION
The AchA is the last branch of the internal carotid artery (ICA) that supplies blood to important brain regions, including the posterior limbs of the internal capsule. Anterior choroidal artery (AchA) aneurysms account for approximately 2-5% of all aneurysms [6,9-11].
Recently, coil embolization has been widely used to treat cerebral aneurysms. However, AchA aneurysms are small and often wide-necked, which can lead to perforation and thromboembolic complications during treatment. Such aneurysms should be treated with caution as they may result in hemiplegia, hemiparesis, and homonymous hemianopsia (3-H). There are only a few reports of AchA aneurysms treated with coil embolization, and all of them do not show the ratio of AchA aneurysms treated with coil embolization. This study reports the treatment results of 92.3% of total AchA aneurysms treated with coil embolization at our institute.
MATERIALS AND METHODS
Population
Aneurysms treated from January 2006, when coil embolization was started at our institute, to March 2022 were included. A total of 104 AchA aneurysms were found in 104 patients; 96 aneurysms (92.3%) were treated with coil embolization, and 8 (7.7%) were treated with aneurysmal neck clipping. There were no significant morphological differences in aneurysms between the coil embolization and aneurysmal neck clipping groups. The data of 96 patients were reviewed using medical records to identify sex, age, rupture, Hunt Hess grade, and modified Rankin Scale (mRS) score. The aneurysm size, laterality, dome-to-neck ratio, aneurysm and AchA location, multiple aneurysms, and lobulation were reviewed using angiograms. The study was approved by the Institutional Review Board (no. 2022-05-028), and formal consent was not required for this type of study.
Characteristics of aneurysms
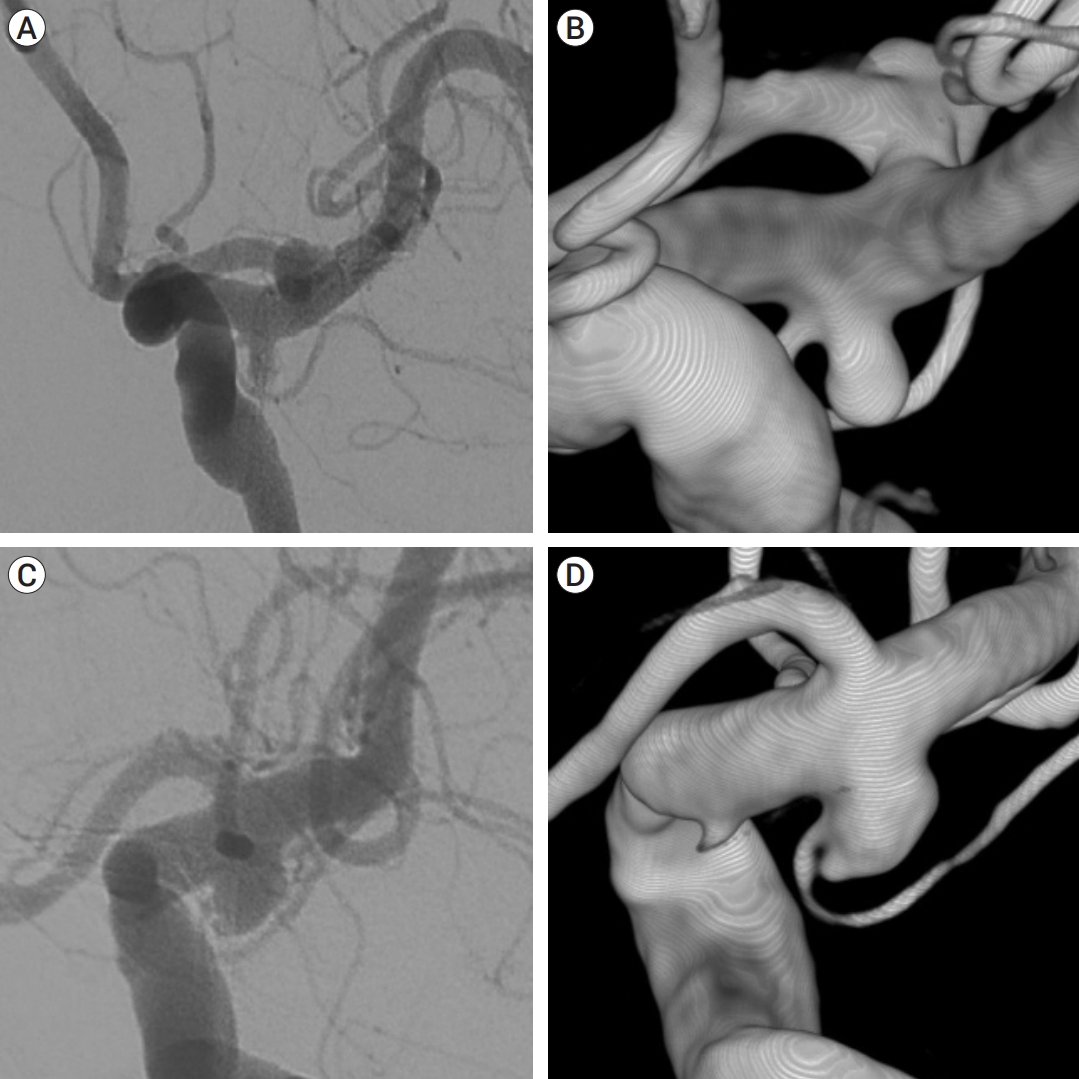
The size of the aneurysm was determined as the maximum length of the sac. An aneurysm with a neck size >4 mm or a dome-to-neck ratio <1.5 was defined as a wide-neck aneurysm. Aneurysm types were classified according to AchA location. Type A aneurysms were classified as originating from the AchA at the junction of the ICA and the aneurysm, and type B aneurysms were classified as originating from the aneurysm neck with a clear gap between the ICA and AchA (Fig. 1) [9].
Endovascular procedure
Except in the very first case, a standardized protocol was used under general anesthesia in all cases. The aneurysm dome, neck size, and depth were confirmed using working angle images. Patients with unruptured aneurysms were pre-medicated with aspirin and clopidogrel for at least five days before embolization. After inserting the sheath, 1000 U heparin was administered every hour after administering 3000 U. Intraarterial tirofiban infusion (0.1-0.8 mg) was administered in case of thromboembolism. The patient who underwent stent-assisted coil embolization took aspirin and clopidogrel for at least 9 months and took aspirin only for the 2 years more.
Angiographic outcome and recanalization
Angiographic outcome was measured using a threepoint Raymond scale (complete occlusion, residual neck, and residual aneurysm) [15]. Initial angiography results were obtained immediately after surgery, and magnetic resonance angiography (MRA) and digital subtraction angiography (DSA) were performed at 6 and 12 months, respectively.
The final angiographic results were confirmed by the final MRA or DSA findings. Comparing the final angiography with the initial outcome, minor recanalization was defined as new or more contrast filling in the aneurysm neck and major recanalization as new contrast filling in the aneurysm dome.
Thromboembolic events included occlusion of the internal carotid, middle cerebral, and anterior cerebral arteries as well as AchA occlusion due to thrombus. Procedurerelated complications were assessed to determine whether they were symptomatic or asymptomatic.
Clinical outcome
The clinical outcome of the patient was assessed using the mRS score at admission and discharge. In patients with thromboembolic events, diffusion weighted image was taken to evaluate the degree of ischemia.
Statistics
All statistical analyses were performed using SPSS for Windows (version 18.0, SPSS, Chicago, Ill, USA). The factors affecting aneurysm recurrence were evaluated. Logistic regression analysis was used for univariate and multivariate analyses. Univariate analyses included the presence of subarachnoid hemorrhage, dome-to-neck ratio, lobulation, multiple lesions, and neck type. Those included in the univariate analysis were included in a multivariate logistic regression model. Statistical significance was set at p<0.05.
RESULTS
Patient characteristics
The study population included 34 men (35.4%) and 62 women (64.6%) with a median age of 61 years (range 22-80 years). A total of 65 unruptured and 31 ruptured AchA aneurysms were treated. Among the ruptured aneurysms, the Hunt Hess grade was I in 3 patients, II in 8 patients, III in 13 patients, IV in 6 patients, and V in 1 patient. Leftsided aneurysms (55 aneurysms [57.3%]) were more common than right-sided aneurysms (41 aneurysms [42.7%]), and 45 patients (46.9%) had multiple aneurysms (Table 1).
Characteristics of aneurysms
The median values of the aneurysm dome size, depth, and neck were 3.7 mm (1.4-13.2 mm), 3.6 mm (1.5-10.3 mm), and 2.7 mm (0.8-8.5 mm), respectively. Wideneck aneurysms were observed in 61 patients (63.5%). Type A was observed in 18 (18.8%) and type B in 78 (81.2%) cases (Table 1).
Initial angiographic outcome and technique of coil embolization
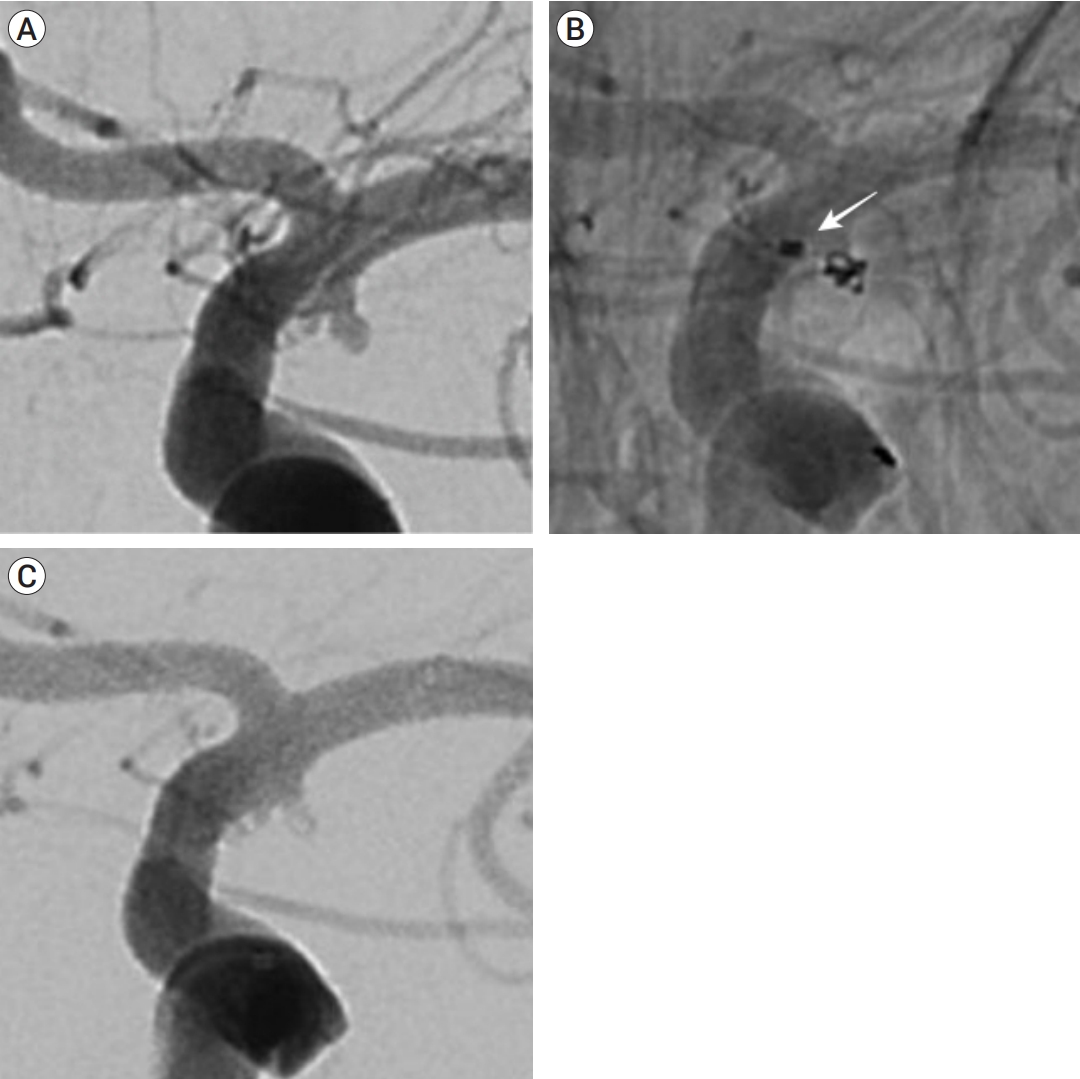
The degree of angiographic occlusion of aneurysms was complete occlusion (Fig. 2) in 41 (42.7%), residual neck in 45 (46.9%), and residual aneurysm in 10 (10.4%) aneurysms. The single-catheter technique was used in 28 cases (29.2%), multiple catheter technique in 46 cases (47.9%), and stent-assisted coil embolization in 22 cases (22.9%). None of the patients underwent balloon-assisted coil embolization.
Procedure-related complications
The only (1.0%) symptomatic procedure-related complication was occurred in the first case of this series. During coil embolization, the guiding catheter was wedged in the ICA, causing blood flow arrest and resulting in left middle cerebral artery (MCA) territory minor infarction.
There were asymptomatic procedure-related complications in four cases (4.2%): one case of contrast leakage from the dome at the end of coil filling and three cases of thromboembolism. All of the events occurred in ruptured cases. The contrast leakage stopped immediately after additional coil insertion. MCA occlusion by thrombus was detected in two cases, and complete recanalization was achieved by mechanical thrombectomy and intraarterial tirofiban injection. In one case, a thrombus was observed in the distal MCA branch, and the distal flow recovered after intraarterial tirofiban infusion only. AchA occlusion did not occur in any of these cases.
Follow-up angiographic outcome
Follow-up angiography was performed in 80 patients (83.3% [MRA, 48; DSA, 32]). The median radiographic follow-up period was 25 months (range 6-174 months). Complete occlusion was the most common (n=57, 71.3%), followed by residual neck (n=22, 27.5%), and residual sac (n=1, 1.3%). Recanalization occurred in 11 cases (13.8%): minor recanalization in 10 cases (12.5%) and major recanalization in 1 case (1.3%). Minor recanalization occurred in five cases (5/20, 25%) of ruptured aneurysms and five cases (5/60, 8.3%) of unruptured aneurysms. Major recanalization was found in one case (1/60, 5%) in the ruptured group, and re-embolization was performed. Risk of recanalization was significantly different between the unruptured and ruptured aneurysms (p=0.012; odds ratio 7.780; 95% confidence interval 1.574-38.447) (Table 2).
Type A aneurysms had minor recanalization in one case (1/14, 7.1%), while type B aneurysms had minor recanalization in nine cases (9/66, 13.6%) and major recanalization in one case (1.5%). Recanalization was higher in type B than in type A, but the differences were not statistically significant.
Clinical outcome
All the unruptured aneurysms had a mRS score of 0 at presentation. The patient with intraoperative left MCA infarction presented with motor aphasia postoperatively and deteriorated to an mRS of 1 on discharge. The patient showed partial improvement later on. In the ruptured group, there were four cases of exacerbation of mRS after coil embolization, one case of vasospasm, and three cases of death due to aggravated cerebral edema, even after decompressive craniectomy.
DISCUSSION
Thromboembolic complications during treatment of AchA aneurysms
Occlusion of AchA during treatment may result in serious complications, including the 3-H syndrome. Viale and Pau reported AchA occlusion after neck clipping of AchA aneurysm in two cases (29%) [17]. Bohnstedt et al. reported that postoperative ischemia occurred in 15 cases (15/112, 12%) after treatment of AchA aneurysms with microsurgical clip ligations and was closely related to the number of temporary clip applications [3]. Friedman et al. reported that AchA territory infarction occurred in 16% (8/51) of their cases and that it could be caused by intraoperative AchA sacrifice, intraoperative thromboembolism, postoperative clip blade distortion due to brain edema, and AchA vasospasm [7]. Recently, Byoun et al. reported that intraoperative neuromonitoring during aneurysmal clipping was able to reduce ischemic complications (6.08%) due to unintentional AchA occlusion [4]. Aoki et al. also reported that no complications occurred in nine patients treated with surgical clipping after the introduction of indocyanine green videoangiography and motor-evoked potential [1].
Kim et al. treated AchA aneurysms with coil embolization and asymptomatic AchA occlusion occurred in 8.1% (3/37) and symptomatic AchA occlusion occurred in 5.4% (2/37) of the aneurysms [11]. In case of AchA occlusion due to thromboembolism during surgery, anticoagulation and antiplatelet agents (heparin, abciximab) were used. In case of vasospasm, flow was restored with papaverine administration [11]. Kim et al. reported that one of the advantages of coil embolization is that blood flow patency can be checked easily during the entire procedure [11]. Kang et al. reported that AchA occlusion occurred in eight cases (8.9%) during coil embolization. In six cases, intraarterial thrombolytic agents (tirofiban, urokinase, and abciximab) were used during surgery, and in one case, the last inserted coil was removed and recanalized [9]. One patient had complete occlusion, but no recanalization was attempted because of retrograde filling of the AchA, and no neurologic deficit occurred. Symptomatic procedure-related complications occurred in three cases (4.4%), but all were transient neurological deficits. Our study is the largest series of AchA aneurysms treated with coil embolization and reports the results of treating 92.3% of total AchA aneurysms with coil embolization at one institution. AchA occlusion was not observed, but symptomatic MCA territory infarction by guiding catheter wedging occurred in one case (1.0%). Moreover, three (3.1%) asymptomatic MCA occlusion were detected, but immediately recanalized. Our results showed that treating AchA aneurysms primarily with coil embolization can achieve good results.
Recanalization of coil embolization of AchA aneurysms
Although coil embolization has several advantages over neck clipping, it is known to result in more recanalization [8,12]. Piotin et al. treated AchA aneurysms with coil embolization, and minor recanalization was observed in 7.1% (1/18) of the cases [14]. In the study by Kim et al., minor recanalization was observed in 10.3% (3/29) and major recanalization in 6.9% (2/29) of the cases. In the study by Kang et al., minor recanalization was observed in 11.9% (8/67) and major recanalization in 3.0% (2/67) of the cases [9,11]. In our study, minor recanalization occurred in 12.5% (10/80) and major recanalization in 1.3% (1/80) of the cases, which is similar to the results reported in previous studies. From these results, it was considered that the durability was good when treating most AchA aneurysms with coil embolization.
Our results showed that the ruptured group had significantly more recanalization than the unruptured group. Raymond et al. reported that ruptured aneurysms showed more recurrence because the complete occlusion rate of coil embolization was low [15]. Park et al. reported that when treating ruptured aneurysms, dense coil packing could not be achieved because the coil was not sufficiently inserted for fear of rupture during surgery. In addition, because antiplatelet agents are not sufficiently used, stent insertion is not preferred because of concerns regarding thromboembolic events. In such cases, staged coil embolization should be considered a treatment option, and short-term angiographic follow-up should be performed [13]. In our results, the recurrence rate was significantly higher (p=0.012) in the ruptured group. In our opinion, because antiplatelet agents or anticoagulants were not sufficiently used, the thrombus developed rapidly during coil insertion, and the packing density was lowered.
Relationship between AchA and aneurysm
Kang et al. classified aneurysms into two types, and all thromboembolic events in their study occurred among type B aneurysms (8/90, 8.9%) [9]. Additionally, Kim et al. classified aneurysms depending on AchA incorporation, and in their report, transient AchA occlusion occurred only in the incorporated group (5/21, 23.8%) [11]. In our series, four cases of thromboembolic events occurred, but all were not related to AchA, and AchA occlusion was not observed at all. The use of tirofiban appeared to have helped prevent the occurrence of AchA occlusion. In our study, there was no difference in thromboembolic events by type; however, there were differences in recurrence. It occurred more frequently in type B, but the difference was not statistically significant (type A: 7.1% vs. type B: 15.2%). We prioritized preservation of AchA rather than dense filling of the coil in the aneurysmal neck, and it is thought that recurrence occurred more in type B.
Flow diverter of AchA aneurysm
Flow diverter is a device that keeps the blood flow of large vessels and perforating vessels while diminishing the blood flow into the aneurysm [5]. Srinivasan et al. reported that they treated 18 cases of AchA aneurysm with a flow diverter, and as a result, there were no AchA occlusion symptoms and no flow change [16]. Bhogal et al. treated 30 cases of AchA aneurysm with a flow diverter; of these, only one patient (3.3%) had a periprocedural embolic ischemic lesion [2]. Given this result, flow diverter can be a good treatment device for AchA aneurysms. However, it still has limitations in that these are small size studies and long-term follow-up was not performed. Therefore, a larger cohort, including long-term follow-up will be required [2,16].
CONCLUSIONS
In this study, most AchA aneurysms were treated with coil embolization at a single institution, and procedure-related complications and follow-up outcomes showed good results compared with previous studies. Therefore, we believe that the coil embolization can be considered a primary option for the treatment of most ruptured and unruptured AchA aneurysms.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






