



INTRODUCTION
During endovascular coiling of cerebral aneurysms [5], intraprocedural rupture (IPR) has a lower incidence but higher morbidity than surgical clipping [3]. IPR is a fatal procedural complication related to morbidity and mortality. The incidence of IPR during coil embolization has been reported to be approximately 5% for ruptured cerebral aneurysms and 1.5% for unruptured cerebral aneurysms [14]. IPR has been independently associated with a severe neurological condition, small, ruptured cerebral, and small bleb-like lesion aneurysms [1,2,4,6,7,9,10,12,14]. However, the relationship between the period of IPR and clinical outcomes remains unknown.
Since endovascular coiling is conducted within the confined space of the skull, Immediate IPR, which introduces additional volume leading to elevated intracranial pressure, is anticipated to pose a greater risk during endovascular coiling compared to microsurgical clipping. Promptly sealing the site of rupture is generally advisable to minimize the risks associated with procedural complications and mortality. Accordingly, contrast leakage period may be a critical factor related to poor clinical outcomes after IPR. This study aimed to retrospectively evaluate the relationship between clinical outcomes and contrast leakage period.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board (IRB No. 2019-01-217). The patientsŌĆÖ medical records and radiographic studies were retrospectively reviewed to obtain clinical and radiographic information from a prospectively recorded aneurysm coiling chart. Data regarding the clinical status of patients lost to clinical follow-up were obtained via telephone. Patients undergoing cerebral aneurysm endovascular treatments of non-saccular aneurysms such as fusiform aneurysms, dissecting aneurysms, blood blister-like aneurysms, traumatic pseudoaneurysms, and mycotic aneurysms were excluded. Patients with flow diversion, multiple stenting without coil packing, proximal occlusion, or internal trapping were also excluded.
In total, 2,859 endovascular coil embolization procedures for 2,683 saccular intracranial aneurysms in 2,501 patients treated at one of two institutions between January 2010 and October 2018 were considered. A total of 1,838 patients (73.5%) were women. The mean age at the time of coil embolization was 59.7 years. A total of 526 cerebral aneurysms (18.4%) were treated with endovascular coiling in ruptured status. A total of 2,412 aneurysms (84.4%) were in the anterior circulation. We defined IPR as the definite extravasation of contrast material on angiography resulting from aneurysm rupture during endovascular coiling. The contrast leakage period, on the other hand, is defined as the duration starting from the moment we initially detected that the microcatheter or coil had exited the artery, or when we first observed contrast leakage, up to the point when cerebral angiography confirmed the cessation of contrast leakage.
Under rupture conditions, the Hunt and Hess grade (HHG) and modified Fisher grade (mFG) were recorded. Clinical outcomes were measured at discharge and the endpoint of clinical follow-up using the modified Rankin Scale (mRS) score. Each patientŌĆÖs clinical status at the final clinical follow-up evaluation was recorded as the follow-up clinical outcome unless there were any aneurysm-related issues. In addition, angiographic outcomes were measured using the Raymond-Roy Occlusion Classification [16].
The maximum diameter of each aneurysm was recorded as the aneurysm size. Coiling technique types were classified as simple, stent-assisted, and balloon-assisted. Simple coiling consisted of either single or multiple catheter techniques. The IPR site was categorized as either the dome or neck of the aneurysm. We defined leakage time as the duration from the onset of IPR to its control through additional coil packing or stenting, as confirmed on angiography. Intraoperative monitoring using motor-evoked potentials (MEPs) and somatosensory-evoked potentials (SSEPs) was routinely performed at one institution.
Conventional or magnetic resonance angiography was used for subsequent imaging to detect aneurysm recurrence. Follow-up imaging was generally performed annually after coil embolization, with results classified into one of three categories: stable or improved occlusion (defined as no change or a decrease in the residual aneurysm), minor recurrence (defined as regrowth or coil compaction of the aneurysmal neck portion), and major recurrence (defined as regrowth or coil compaction of the aneurysmal sac requiring retreatment).
Patients were divided into the following two groups of equal number based on contrast leakage period: long contrast leakage period group (LCG, Ōēź10 min) and short contrast leakage period group (SCG, <10 min). We compared between-group differences in various parameters. Data were analyzed to assess potential correlations between the duration of contrast leakage and clinical parameters. The following parameters were compared between the SCG and LCG groups: age, aneurysm size, gender, prior rupture status, intravenous heparin administration, coiling technique, IPR location, microcatheter protrusion, immediate radiological outcomes, immediate CT findings, extraventricular drainage, ventriculoperitoneal shunt placement, retreatment, IPR onset, mRS score at discharge, and mRS score.
Endovascular strategies
Endovascular coiling is generally performed under general anesthesia. Biplane angiographic units (Integris Allura 12/12, Philips, Netherlands, or Artis Zee Biplane System, Siemens, Munich, Germany) were used. In cases of rupture, oral antiplatelet agents were not used before coil embolization, and intravenous heparin (a bolus of 3,000 IU) was administered either to achieve microcatheter super selection of the aneurysm or after the aneurysm was secured with a coil. In unruptured cerebral aneurysms, dual oral antiplatelet agents (75 mg clopidogrel and 100 mg aspirin) were administered for 5 days before endovascular coiling, or a loading dose was administered (300 mg clopidogrel and 100 mg aspirin). After attaining access to the femoral artery, a 3,000-5,000 IU heparin bolus was administered intravenously, according to the patientŌĆÖs weight. An additional 1,000 IU heparin bolus was administered hourly to maintain an activated clotting time of >250 s. Excelsior SL-10 (Stryker Neurovascular, Fremont, CA, USA), Echelon 10 (Medtronic, Irvine, CA, USA), or Headway17 (Microvention, Tustin, CA, USA) coil-delivery microcatheters were used. Target (Stryker Neurovascular, Fremont, CA, USA), Axium (Medtronic, Irvine, CA, USA), and Microplex (Microvention, Tustin, CA, USA) detachable coils were used. When stent-assisted coiling was necessary, Enterprise (Codman & Shurtleff, Raynham, MA, USA) and Neuroform (Stryker Neurovascular, Fremont, CA, USA) stents were used. The HyperGlide Occlusion Balloon System (Medtronic, Irvine, CA, USA) was used for balloon-assisted coiling. If an antiplatelet drug was necessary, aspirin (100 mg) or dual antiplatelet therapy (100 mg aspirin and 75 mg clopidogrel) was administered for 3-6 months after coil embolization.
Intraoperative neuromonitoring
The Eclipse system (Medtronic, Memphis, TN, USA) was used for stimulation and data recording. For SSEP monitoring, the lower-extremity median nerves of the upper and posterior tibial nerves were stimulated using surface electrodes. A 200-╬╝s, square-wave electrical pulse was presented sequentially to the bilateral median and posterior tibial nerves at a frequency of 2.31 Hz with a stimulation intensity ranging from 18 to 23 mA. Recording needle electrodes were placed at C3ŌĆ▓ (2 cm posterior to C3), C4ŌĆ▓ (2 cm posterior to C4), CzŌĆÖ, and Fpz according to the international 10-20 system of electrode placement. To determine MEPs, needle electrodes were placed at C3, C4, and Cz for stimulation. Trains of eight biphasic pulses with an interstimulus interval of 0.75 ms were delivered at a rate of 1 Hz. The stimulation intensity ranged from 350 to 450 V. Compound action potentials were recorded from the abductor pollicis, vastus, anterior tibialis, and abductor hallucis muscles. Baseline SSEPs and MEPs were obtained after anesthetic induction. SSEPs were monitored continuously throughout the operation, and MEPs were obtained just before the beginning of the critical interventional procedure (e.g., coil insertion), after the end of each procedure (e.g., each coil packing), after the end of the entire procedure, before removal of the femoral sheath, and additionally according to the surgeonŌĆÖs judgment. Alarming values were defined as an SSEP or MEP decrease of more than 50% amplitude and/or a 10% latency increase. Changes were classified as permanent if they did not return to baseline before the end of the operation [11].
Statistical analysis
Statistical analyses were performed using SPSS for Windows version 27 (SPSS, Chicago, IL, USA). Clinical outcomes were dichotomized as good (modified Rankin Scale [mRS], 0-2) or poor (mRS, 3-6). Factors related to contrast leakage period at IPR were evaluated. Chi-squared tests or FisherŌĆÖs exact tests were used to analyze categorical variables, while the StudentŌĆÖs t-test or Mann-Whitney U test was used for continuous variables. Statistical significance was set at p<0.05, with a 95% confidence interval.
RESULTS
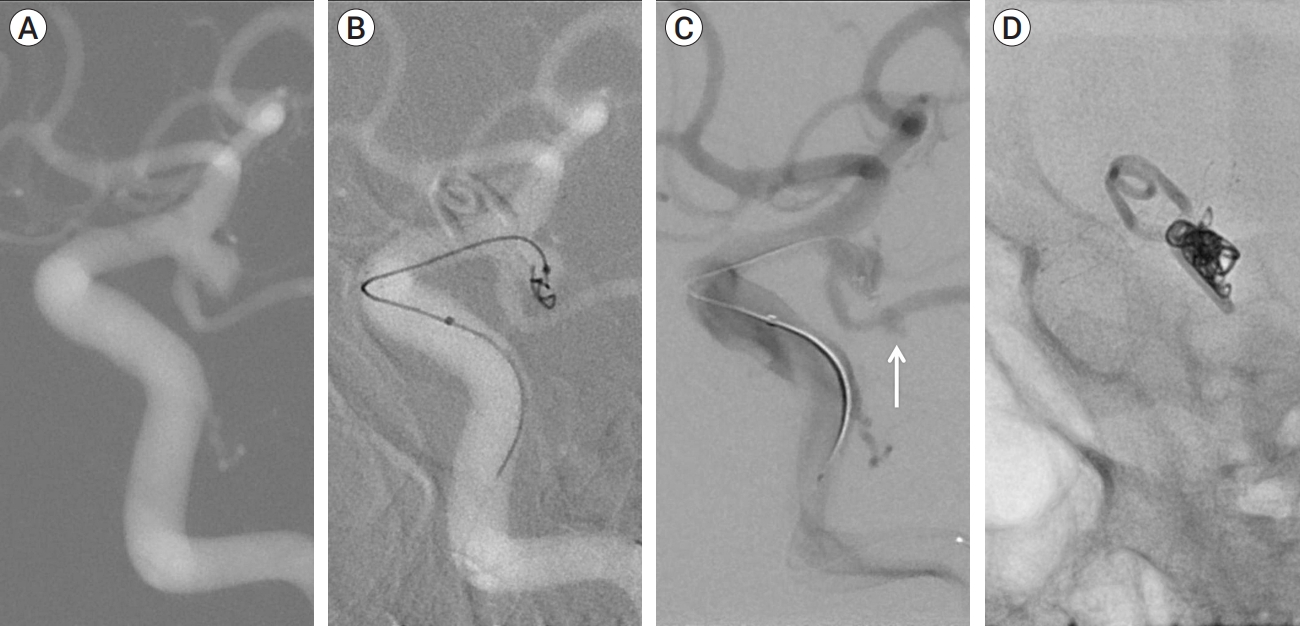
A total of 2,859 cerebral aneurysms were treated with endovascular coiling. Among the study population, IPR occurred in 18 cases (0.63%). Specifically, IPR was observed in 10 cases (1.9%) with ruptured cerebral aneurysms and in eight cases (0.34%) with unruptured cerebral aneurysms. Twelve patients with IPR were female, with a mean age of 56.3 years (range: 26-76 years). The mean aneurysm size was 4.51 mm, ranging from 2.3 to 7.52 mm. The most common IPR location was the anterior communicating artery (n=9). Furthermore, aneurysms occurred in middle cerebral artery lesions (n=2), posterior communicating arteries (n=3), anterior choroidal arteries (n=1), distal internal cerebral arteries (n=2), and posterior circulation (n=1, ostium of posterior inferior cerebellar artery). For coil embolization, IPR occurred during simple (n=9), stent-assisted (n=8), and balloon-assisted coiling (n=1). IPR developed throughout the procedural steps of initial frame coiling (n=4), coil packing (n=5), stent deployment (n=7), ballooning (n=1), and microcatheter removal (n=1) (Fig. 1). IPR sites included the dome (n=14) and neck (n=4) of aneurysms. Demographic features of patients and procedural findings are summarized in Table 1.
All IPR cases were controlled with additional stenting (n=2) or further coil packing without proximal balloon occlusion. The mean contrast leakage period was 11.2 min, ranging from 1 to 31 min. The immediate radiologic outcomes were complete (n=10), residual neck (n=6), and residual sac (n=2). CT scans performed immediately after IPR showed new subarachnoid hemorrhage (in the unruptured aneurysm, n=8), hydrocephalus formation (n=1), and subarachnoid hemorrhage (SAH) increase (n=5), with no case of mass effect caused by intracerebral hemorrhage.
Post-procedure temporary external ventricular drainage was performed in 6 patients (33.3%), five with ruptured and one with unruptured aneurysms, to control increased intracranial pressure (IICP) or acute hydrocephalus. A permanent ventriculoperitoneal shunt was placed in two patients with subarachnoid hemorrhage. Four IPR patients underwent endovascular coiling under intraoperative neuromonitoring (IONM). A decrease in SSEP amplitude and subsequent decrease in MEP were detected in all patients with IPR under IONM. IONM eventually showed MEP recovery and normalized SSEP amplitudes after IPR control (Fig. 2).
Clinical follow-up was possible in all patients with IPR, with a mean follow-up duration of 34.9 months (range: 7 to 91 months). Further, there was no rebleeding of any cerebral aneurysms with IPR. Transient focal neurological deficits developed in two patients, all suffering from motor weakness (grade IV) after IPR. At the end of clinical follow-up, 14 patients had an mRS score of 0, three had an mRS score of 2, and one had an mRS score of 4. Eight patients with unruptured cerebral aneurysms had no permanent neurological defect after IPR.
Follow-up imaging data were accessible for 16 patients (88.9%), with a mean time interval between coiling and the most recent follow-up image of 24.8 months. Among these, two patients (12.5%) experienced major recurrence following IPR, occurring at 1 and 6 months after endovascular coiling. Flow diversion was performed using a flow diverter, FRED (Microvention, Tustin, CA, USA), in one IPR case and surgical clipping in the other.
Mean contrast leakage periods for the SCG and LCG were 5.22 min (range: 1-9 min) and 17.11 min (range: 10-31 min), respectively. Ruptured aneurysms were frequent in the SCG (77.7% versus 33.3% for SCG versus LCG, p=0.153). Microcatheter protrusion into the subarachnoid space was frequent in the LCG (0% versus 44.4% for SCG versus LCG, p=0.082). Extraventricular drainage was frequently required to treat SCG versus LCG patients (55.5% versus 11.1%, respectively; p=0.131); however, permanent cerebrospinal fluid (CSF) diversion was infrequent (22.2% versus 0, respectively; p=0.471). There was no evidence of a statistical between-group difference in clinical outcomes (Table 2).
DISCUSSION
IPR is regarded as a potentially fatal procedural complication and is associated with poor clinical outcomes. Additionally, IPR during coil embolization tends to be associated with better clinical outcomes than spontaneous aneurysm rupture [2,7]. In our series, all cases of IPR were controlled and produced relatively good clinical outcomes. Additionally, patients with unruptured cerebral aneurysms who underwent IPR had no permanent focal neurological deficits. We suggest that clinical outcomes may not be poor after controlling for IPR.
Since early rebleeding risk exists even after coil embolization of ruptured cerebral aneurysms [8], rebleeding might be possible in cerebral aneurysms that underwent IPR during endovascular coiling. However, in this study, there were no cases of early rebleeding after IPR. IPR is generally controlled with further coil packing from outside the aneurysm into the aneurysm sac; however, ruptured cerebral aneurysms are treated with coil packing within the aneurysm sac. Additionally, during the procedure, the cerebral aneurysm with IPR tends to be filled densely with coils. This difference in coil packing between aneurysms with IPR and ruptured cerebral aneurysms may explain the low rebleeding risk associated with IPR in our series.
We hypothesized that clinical outcomes might be poor in patients with a contrast leakage period of >10 min. However, there was no significant difference in clinical outcomes in our series when LCG (n=9) and SCG (n=9) were compared. All patients in our series were controlled within approximately 30 min after IPR. Although a time limit for contrast leakage period may exist based on the Monro-Kellie doctrine, cases of IPR in our series controlled within 30 min showed relatively good clinical outcomes. Accordingly, we suggest a minimal requirement for avoiding poor clinical outcomes in IPR is their control within 30 min.
Surgeons treating IPR cannot predict clinical outcomes even after controlling for IPR before the patient is weaned off general anesthesia. Therefore, IONM recovery may be correlated with good clinical outcomes after IPR [17]. In our series, all patients with IPR under IONM surveillance (n=4) had significantly decreased SSEP amplitude, followed by a significant decrease in MEPs. After IPR control, IONM first revealed MEP and then SSEP recovery. It is known that SSEPs may be related to cortical function, and MEPs may be related to subcortical function [11,13,15]. Therefore, if ICP is increased in IPR, the cortical function may first decrease. However, if IICP is controlled, the cortical function may recover rapidly. Therefore, we suggest that recovery of SSEP amplitude may be an effective tool for achieving good clinical outcomes after controlling for IPR.
Limitations of our study include its retrospective design, causing vulnerability to selection bias, the small sample size, and the inability to investigate the relationship between IPR period and clinical outcomes with statistical significance. While contrast leakage time might not accurately reflect actual bleeding time, it can be a realistic indicator of bleeding time. A multicenter study is needed to obtain sufficient IPR cases for assessing the relationship between IPR period and clinical outcome.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






