Subdural Hematoma without Subarachnoid Hemorrhage Caused by the Rupture of Middle Cerebral Artery Aneurysm
Article information

Abstract
Pure subdural hematomas caused by a ruptured intracranial aneurysm are extremely rare. We describe the case of a 42-year-old woman who presented with headache without evidence of head trauma. Magnetic resonance angiography and conventional cerebral angiography revealed a ruptured aneurysm at the right middle cerebral artery bifurcation. The patient underwent surgical treatment and had a good outcome without any neurological deficit. The mechanisms and clinical characteristics of this condition are discussed.
INTRODUCTION
In most cases, subdural hematomas (SDHs) are caused by head trauma.7)33) Spontaneous SDH is an uncommon condition, found in only 2.6% of acute subdural hematoma (ASDH) cases. Underlying etiologies for spontaneous SDH include ruptured aneurysms with or without concomitant subarachnoid hemorrhage (SAH), arteriovenous malformations, meningiomas, dural metastatic diseases, and hematologic or solid neoplasm.7)
Spontaneous pure ASDH without concomitant SAH due to the rupture of a cerebral aneurysm is extremely rare and only 40 cases were reported between 1981 and 2012.9)23)35) We report a case of spontaneous ASDH without evidence of SAH caused by a ruptured aneurysm at the middle cerebral artery (MCA) bifurcation, presenting with repeated sentinel headaches.
CASE REPORT
A 42-year-old woman was admitted to our institution with a history of sudden onset headache without any accompanying neurological deficit. A week prior to admission, the patient experienced two episodes of transient headache, each lasting a few hours. She had noted occasional headaches over the last few years; however, they did not last more than a few minutes and were not severe. She had no definite history of head trauma, hypertension, or coagulopathy.
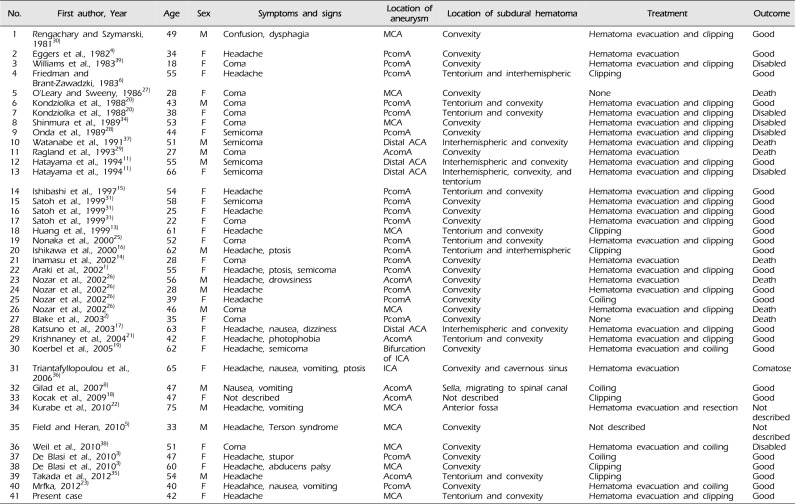
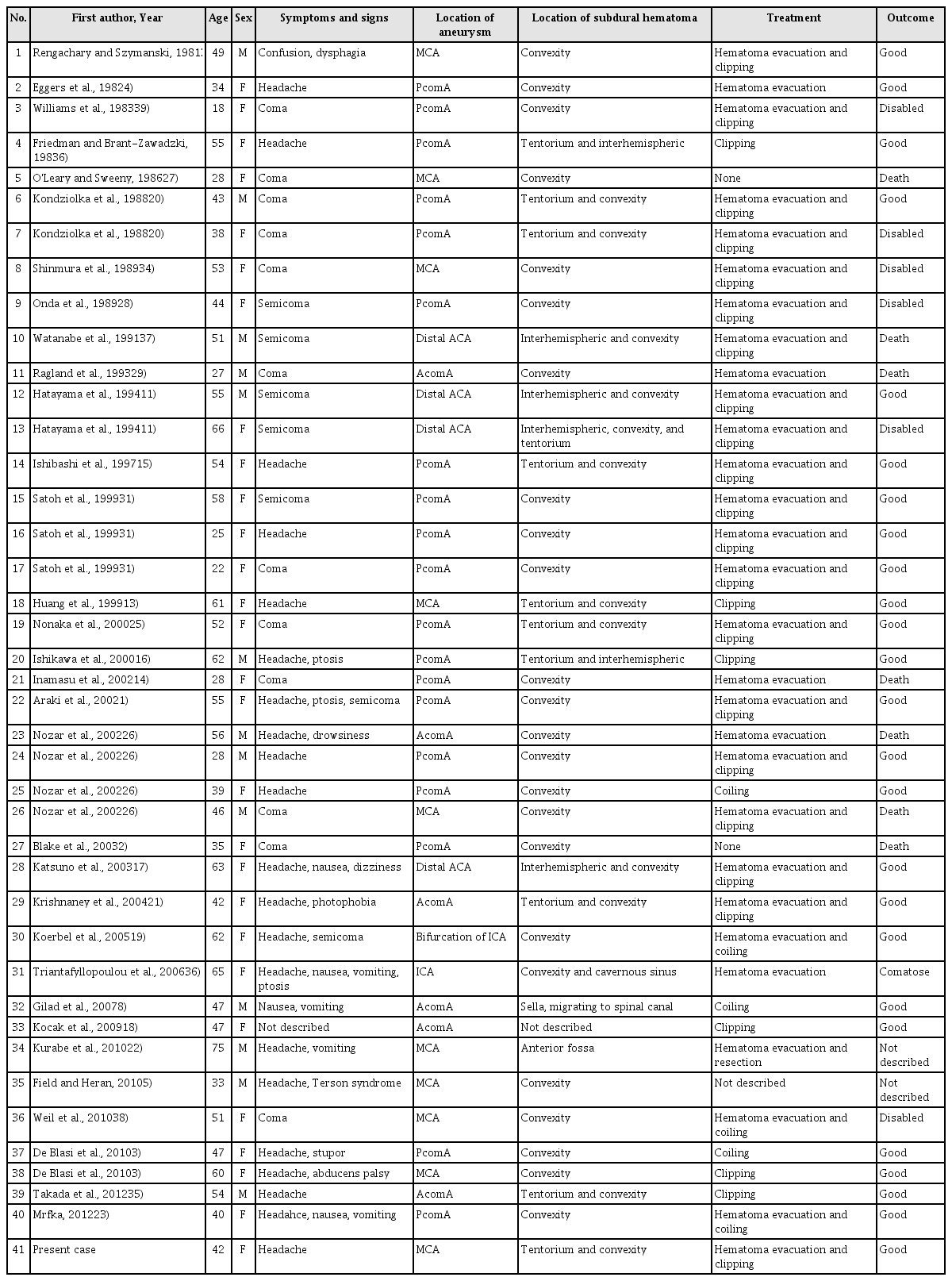
The initial computed tomography (CT) scan of the brain revealed an ASDH without evidence of any other type of hemorrhage including SAH (Fig. 1), and laboratory studies, including coagulopathy screening, showed no abnormalities. For further evaluation, magnetic resonance angiography (MRA) and subsequent conventional cerebral angiography were conducted, revealing a right middle cerebral artery bifurcation aneurysm (Fig. 2).

Initial brain imaging findings of case. Computed tomography scans (A, B) shows no evidence of subarachnoid hemorrhage at the basal cistern and the sylvian fissure and there is only acute subdural hematoma on the right fronto-temporo-parietal area.

Magnetic resonance angiography (A, B; white arrows) and conventional cerebral angiography (C, D; white arrows) show the presence of the right middle cerebral artery bifurcation aneurysm extending antero-inferiorly and laterally.
An aneurysmal neck clipping surgery was performed on the second day of hospitalization. A right pterional approach was used as usual, but when a semi-lunar shaped dural incision was made, only a dark bloody SDH without SAH was noted. There was no discoloration of brain parenchyma; no hematoma was observed in the subarachnoid space. After total removal of the SDH, sylvian fissure dissection was performed and the aneurysm was identified at the middle cerebral artery bifurcation. The aneurysmal dome extended antero-inferiorly and laterally and was tightly adherent to the arachnoid membrane (Fig. 3). Postoperative CT revealed resolution of the ASDH without any complications related to the surgery. The patient's hospitalization was uneventful and a follow-up three-dimensional CT angiography performed 1 year after the operation showed no remnant or recurrent aneurysm (Fig. 4).

Intraoperative photographs shows the aneurysmal sac penetrating into subdural space (A; white arrow). Permanent 7 mm straight mini-clip was introduced to the neck portion of the aneurysm successfully (B).
Follow-up computed tomography angiography 1-year after the operation. The clip is observed in the source image of the computed tomography angiography (A), and there was no evidence of the remnant aneurysm (A, B).
DISCUSSION
The mechanism of ASDH caused by rupture of an intracranial aneurysm is different from that of ASDH caused by trauma and tearing of cortical and bridging veins.10) According to previous studies, various mechanisms have been suggested to explain the occurrence of ASDH without SAH after aneurysm rupture. First, previous repeated minor ruptures of the aneurysm occur, causing small bleeds and the formation of tight adhesions between the aneurysm and the neighboring arachnoid membrane. Eventually, massive bleeding fills the subdural space directly after a major rupture occurs.8)16)23)25) Second, massive high-pressure bleeding causes laceration of the arachnoid membrane with bleeding into the subdural space.8)14)15)16)18) Third, the rupture of a subdural carotid artery aneurysm results in a pure ASDH.12)15)24) Fourth, the cavernous sinus wall is eroded by the acute enlargement of an intracavernous aneurysm after thrombosis, leading to pure ASDH.18)35)
In the present case, intraoperative findings revealed a tight adhesion between the aneurysmal dome and the arachnoid membrane. The patient reported recurrent episodes of sentinel headache, suggesting that repeated small bleedings led to formation of the tight adhesion. These findings are consistent with the first mechanism described above.
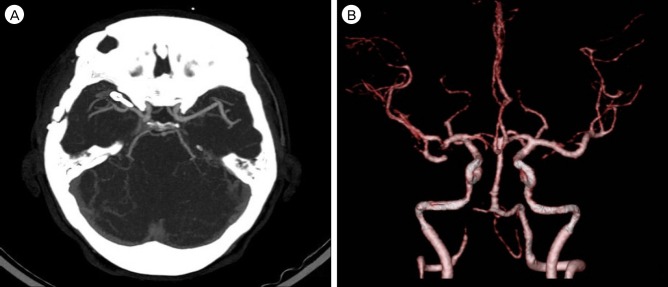
Including the present case, we analyzed 41 cases reported with pure ASDH caused by the rupture of an intracranial aneurysm and have summarized them in Table 1. Of these, 10 were caused by the rupture of an MCA aneurysm, including the present case. In those cases, ASDH was located at the convexity in seven cases, at both the tentorium and convexity in two cases (including the present case), and at the anterior fossa in one case. Six of these 10 cases underwent hematoma evacuation and clipping, as in the present case, and two cases underwent clipping only. In one case, surgery could not be performed, and in another case, treatment was not described. These 10 cases presented with a variety of symptoms and signs and experienced different outcomes. Four cases were comatose at admission, and, in these patients, the final outcomes were poor; two patients died and the other two patients were disabled. The other six cases presented with an alert to confused mental status with headache and/or other minor neurological deficits; in four cases, the final outcomes were reported to be good, and there was no description of outcome in the other two cases.
Cases of pure acute subdural hematoma caused by the rupture of intracranial aneurysm
Among all 41 cases analyzed, 17 patients presented with a semi-comatose to comatose mental status on admission, and only five of these patients (29%) had good outcomes. Six patients died and another six patients were disabled. The remaining 24 cases with a relatively good neurological status had generally good outcomes. Excluding two cases without outcome description, 91% (20/22 patients) had good outcomes, one patient died, and one patient remained comatose. Based on these results, it appears that a favorable neurological status at admission is a predictive factor for a good outcome. These findings are consistent with those of Schuss et al. who studied patients with ASDH and SAH, and concluded that a good neurological status at admission is a predictive factor for a good outcome.32)
CONCLUSION
The rupture of an intracranial aneurysm may be the cause of a pure ASDH in patients without a history of trauma, but this is often mistakenly ruled out because of the absence of SAH. Subsequently, determining the correct cause and providing the proper treatments in these patients may be delayed.
Therefore, when a patient presents with a pure SDH without a history of trauma or coagulopathy, imaging studies, such as three-dimensional CT angiography or MRA, should be performed to evaluate for vascular lesions to determine the underlying cause and to guide optimal treatment for the patient.
Notes
Disclosure: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.