



INTRODUCTION
Coil embolization has become the mainstream treatment for aneurysm and there are two major complications to be avoided, intraprocedual aneurysmal rupture and thromboembolism. Early detection and management is crucial. Thromboembolism usually causes weakness, aphasia, etc., and uncommon neurologic signs can cause confusion during management decisions. Therefore, knowledge about the unusual neurologic deficit caused by thromboembolism will be important to clinicians. We report a case of a rare complication, hemiballism, caused by thromboembolism after coil embolization.
CASE
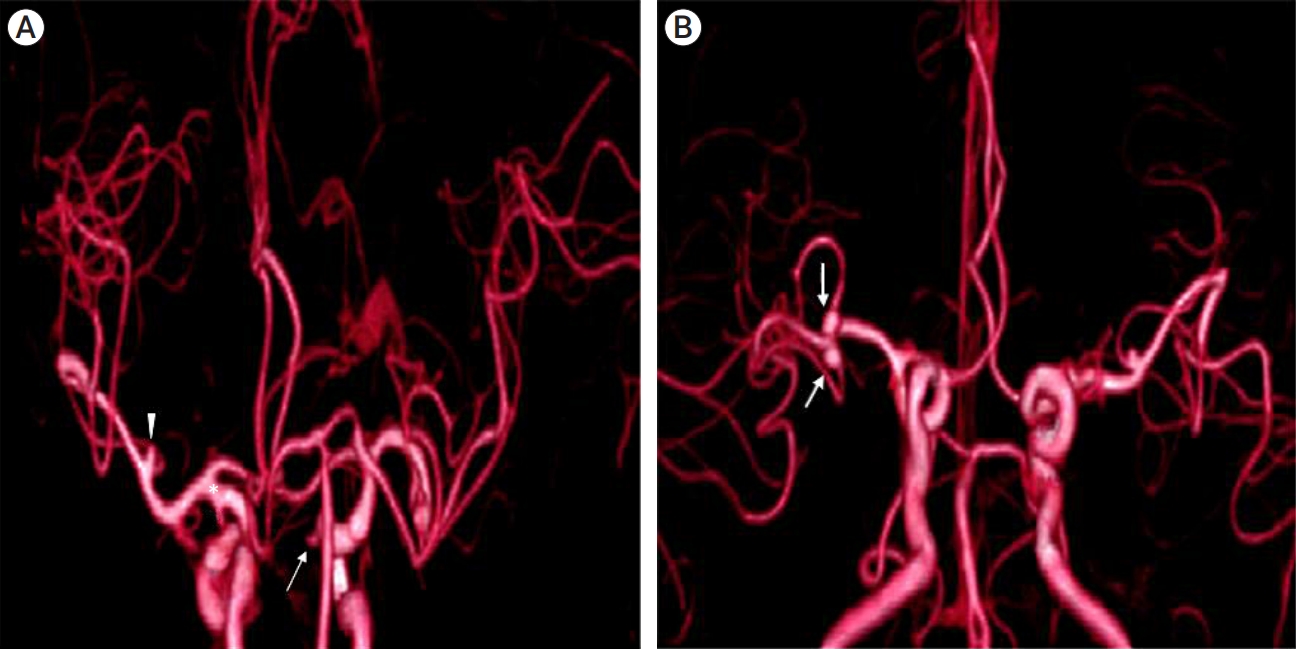
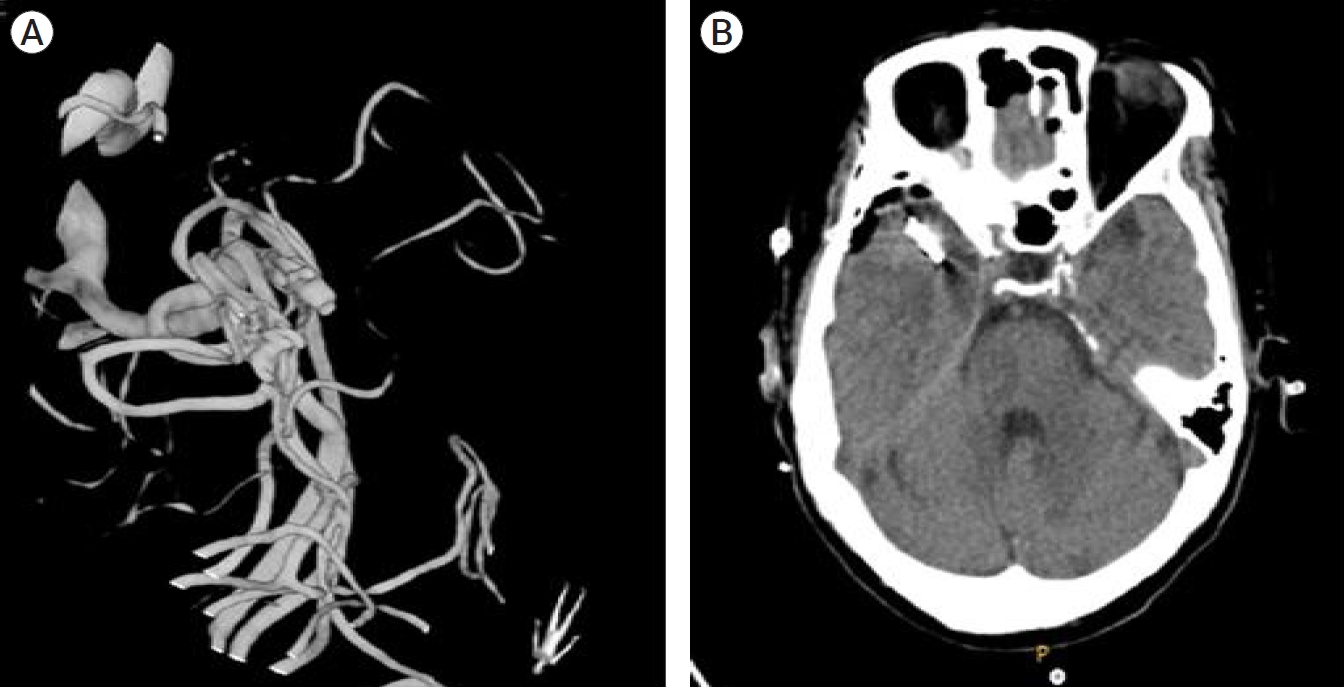
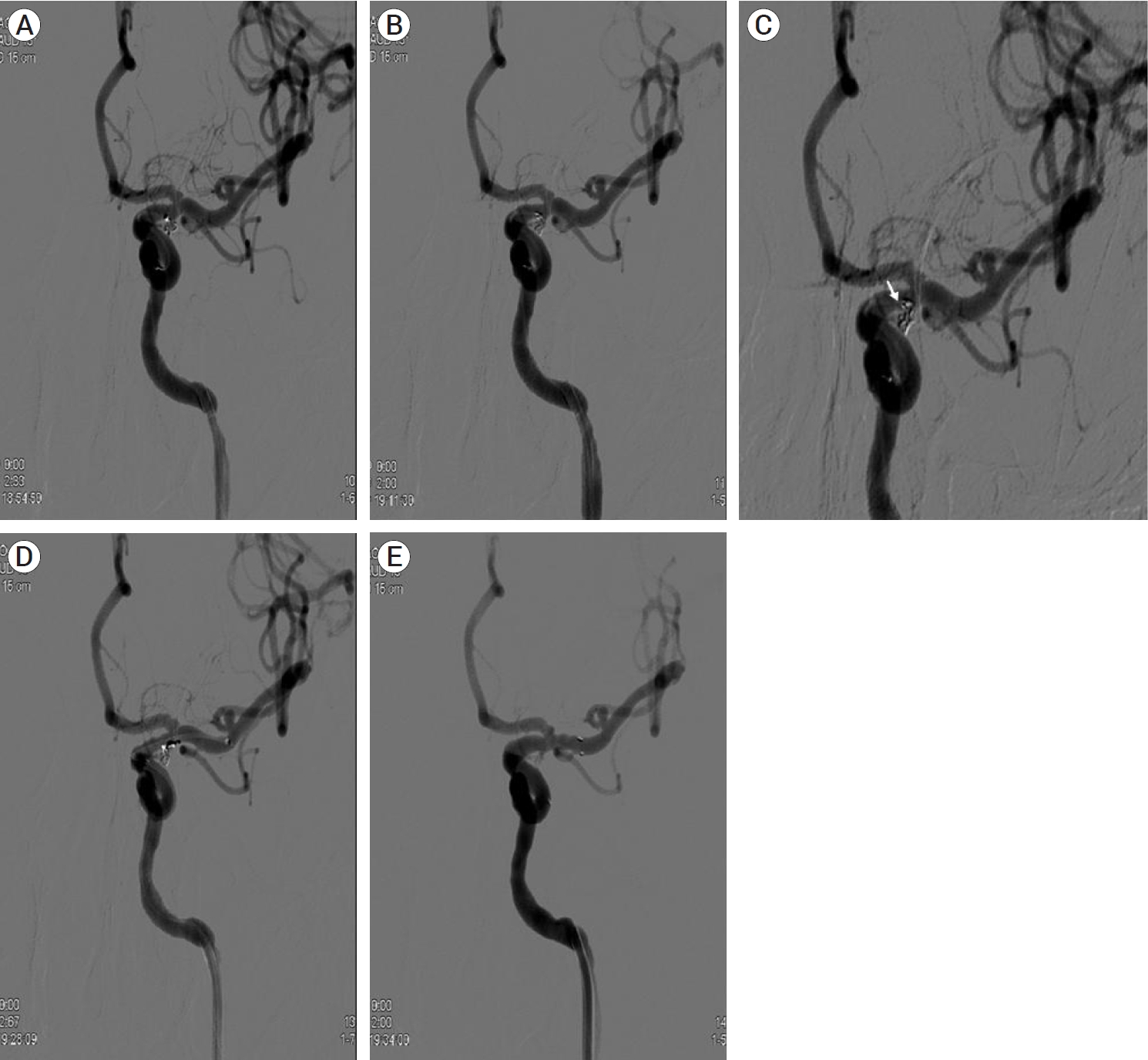
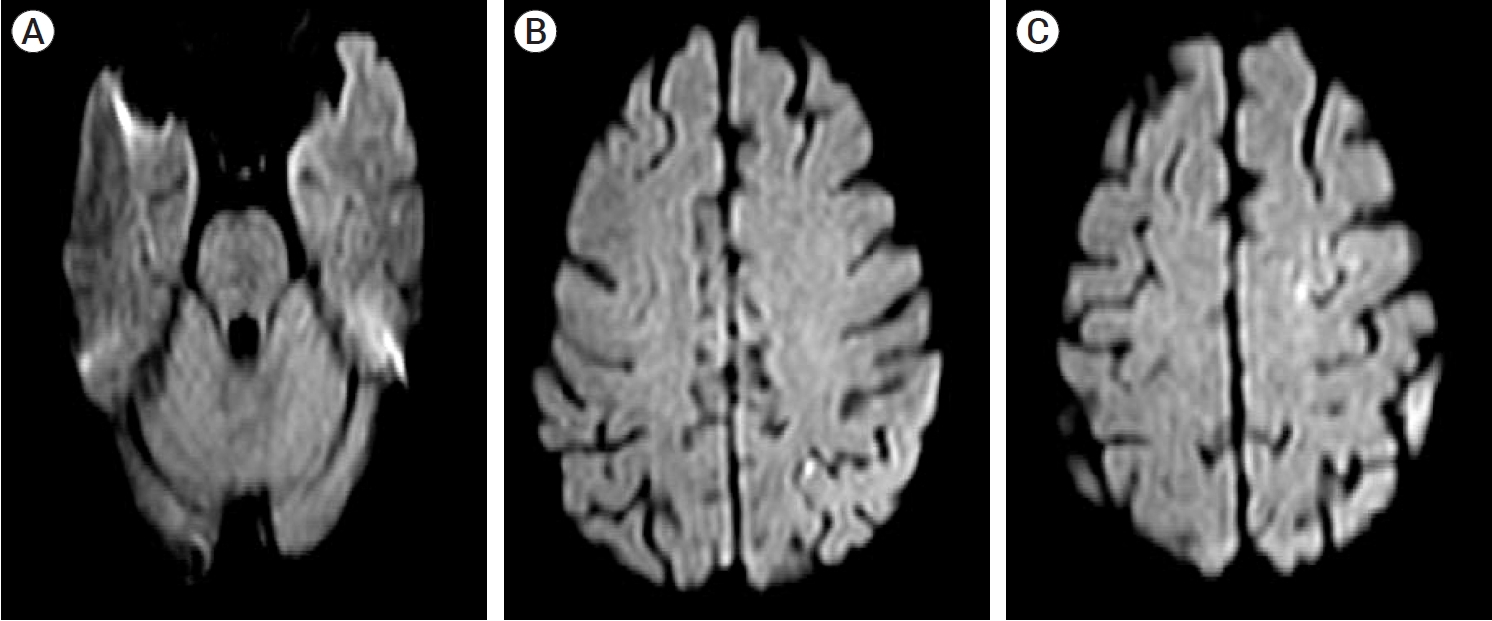
A 69-year-old woman visited our hospital with a vasovagal syncope. Brain computed tomography (CT) and brain computed tomography angiography (CTA) were performed for work up and two unruptured aneurysms on the right middle cerebral artery (MCA), unruptured aneurysms on the right paraclinoid carotid artery and the left posterior communicating artery (pcom), and a left MCA bifurcation were incidentally found (Fig. 1). On conventional angiogram, the sizes of the aneurysms were small but the right MCA and left pcom aneurysms had an irregular shape (Fig. 2) and after counseling with the patient, treatment for the right MCA and left pcom unruptured aneurysms was decided. The two right MCA unruptured aneurysms had a large neck, not suitable for coil embolization, so aneurysmal neck clipping was performed (Fig. 3). The left pcom unruptured aneurysm was decided for coil embolization. On coil embolization, selecting the aneurysm with the microcatheter (Headway microcatheter, MicroVention, Tustin, CA, USA) was difficult because there was an acute angle for entrance to the pcom aneurysm. After shaping the microcatheter into a ŌĆśUŌĆÖ shape and withdrawing the microcatheter from distal to the entrance of aneurysm, aneurysm selection was possible. An Axium (ev3, Medtronic, Irvine, CA, USA) 3D 1.5 mm/2 cm coil was employed as a framing coil, and one additional coil insertion was done (Fig. 4A, B). When a third coil packing was attempted, unfortunately, the microcatheter was unstable and it was dislodged from the aneurysm and a loop of a coil which was deployed inside the aneurysm, herniated to the parent artery (Fig. 4C). The risk of coil herniation appeared to increase with additional coil packing, so further coil packing was halted. To stabilize the herniated coil loop, a Solitaire stent (ev3, Medtronic, Irvine, CA, USA) was deployed and the herniated loop of coil was stabilized to the arterial wall by the stent. The aneurysm was not completely packed, but the bleb was covered, and in the interest of risk-benefit, the procedure was stopped (Fig. 4D, E). Immediately after the procedure, the patient showed global aphasia and right hemiparesis. Diffusion magnetic resonance imaging (MRI) showed small, multiple scattered infarctions on the left frontal, temporal, and parietal cortex, supposedly due to microemboli during the procedure (Fig. 5A-C). Aspirin (100 mg) and plavix (75 mg) were given daily after procedure. Five days after the procedure, aphasia and hemiparesis improved, but the patient complained of numbness on her right hand and intermittent hemiballistic movement on the right arm and leg developed thereafter. Upon examination, there were involuntary, irregular, violent flinging movements, predominantly on her right arm than her right leg, and on the next day, involuntary movement on her leg disappeared but persisted on her arm and numbness had subsided. Follow up diffusion MRI was performed, revealing no significant change of multiple scattered infarctions which were noted on the postoperative diffusion MRI. An electroencephalogram (EEG) was negative for epileptiform discharges and the patient had no family history of movement disorder. Anticonvulsants (valproic acid) and clonazepam were given to the patient empirically, and after 15 days, hemiballism was fully recovered, and the patient was discharged home with no neurologic deficit. Valproic acid and clonazepam were given for about one month and stopped. No more episodes of hemiballism or any other neurologic deficit have occurred since.
DISCUSSION
Hemiballismus is a hyperkinetic movement disorder characterized by involuntary, irregular, large amplitude, violent flinging movements of the limbs. It usually involves the arm, leg, proximal in most cases, occurring with activity which subsides on rest and sleep [7].
Stroke is the most common etiology causing hemiballismus, but stroke-related movement disorders themselves are rare conditions. In the Lausanne stroke registry, hyperkinetic movement disorders were seen in only 1% of the patients with stroke [2]. Other reported cases causing hemiballismus include traumatic brain injury, nonketotic hyperglycemic coma, amyotrophic lateral sclerosis, tuberculomas, vascular neoplasms, systemic lupus erythematosus, systemic vasculitis, and demyelinating plaques [7].
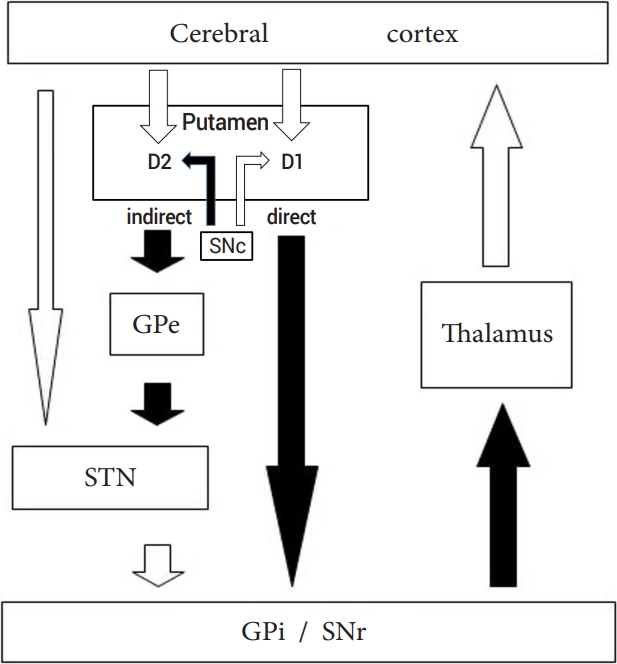
Normally in the extrapyramidal pathway, the thalamus activates the cortex, and the proposed pathophysiology of these hyperkinetic movement disorders is the interruption in the cortico-striato-pallido-thalamo-cortical feedback loop leading to disinhibition of the thalamus, resulting in excessive movement, and a hyperkinetic movement disorder (Fig. 6). The subthalamic nucleus (STN) was classically reported to be the main lesion, but there are reports involving lesions outside the STN, such as cortical and subcortical lesion, basal ganglia, and the thalamus [2].
Morigaki et al. reported two cases of hemiballismus supposedly due to disrupted hemodynamics in the watershed zone to the frontal lobe, which improved after revascularization [4]. In another case, the involuntary movement was caused by the mass effect of a hematoma on the corpus callosum resulting from the rupture of an aneurysm of the distal accessory anterior cerebral artery. They suggested the hyperkinetic movement disorder was by the mass effect of the hematoma interrupting the cortico-striatopallido-thalamo-cortical feedback loop passing through the corona radiata just lateral to the corpus callosum [3]. Sakai K et al. reported chorea occurring eight days after subarachnoid hemorrhage which was explained by decreased blood flow by vasospasm and hydrocephalus inducing interruption of the extrapyramidal feedback loop [5].
Therefore, it appears that a lesion anywhere influencing the extrapyramidal pathway to induce disinhibition of the thalamus could result in hyperkinetic movement disorders.
In our case, after coil embolization, there were small, multiple scattered infarctions on the left frontal, temporal, and parietal cortices which were the suggested lesions inducing the hemiballism. Immediately after the procedure, there was typical ischemic neurologic deficit, such as right hemiparesis and aphasia, and after five days, these neurologic deficits improved and progressed to hemiballisim. The pathophysiology of the delayed onset of hemiballism is not well known. The explanation has been hypothesized as the changes in central nervous system (CNS) plasticity after injury and the re-establishment of functional synapses between the injured CNS neurons and their target cells which results in disinhibition of the thalamus, producing hyperkinetic movement [6].
Antidopaminergic medication can be considered for severe or recurring symptoms. Typical neuroleptics (haloperidol, perphenazine) or atypical antipsychotics (risperidone, clonazepam) may be used and when a long-term therapy is required, catecholamine-depleting agents such as reserpine and tetrabenazine may be considered. In most cases, symptoms tend to subside allowing withdrawal of drugs [7].
Hemiballismus by strokes is classically caused by infarction involving the subthalamic nucleus, but pure cortical strokes are rare. However, the prognosis is better in patients with cortical strokes, which subside more frequently than strokes of other sites [1]. In this case, the patient took valproic acid and clonazepam and the symptoms subsided after 15 days, however, it is not certain if the symptoms recovered spontaneously or improved by medication. However, if involuntary movement symptoms occur after interventional procedures which are caused by microemboli at the cortical area, the prognosis will be good.
CONCLUSIONS
Movement disorders such as hemiballism after interventional therapy are rare, but it can occur as a complication of thromboembolism. Medications such as atypical antipsychotics, etc. can be used however, symptoms tend to subside, especially when it is caused by microemboli at the cortical area allowing withdrawal of drugs.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






