



INTRODUCTION
Pial arteriovenous fistula (PAVF) is an extremely rare condition, accounting for less than 2% intracranial vascular malformations. They can be congenital or results from iatrogenic or traumatic injury. Considering the fact that direct arteriovenous shunt results in high venous blood flow and varix formation with the subsequent risk of haemorrhage, these pathologies need to be treated on most occasions, either by endovascular or microsurgical approach. We encountered a 49-year-old gentleman with complex right middle cranial fossa PAVF with feeders from a single right orbitofrontal middle cerebral artery (MCA) branch with an aneurysm, direct shunting into the basal vein of Rosenthal (BVR) which harboured a venous varix at the origin. When patient returned for treatment, baseline angiogram showed complete occlusion of PAVF. We postulate contrast-induced vasculopathy as a possible cause. To the best of our knowledge, spontaneous occlusion of PAVF was documented only four times in English literature, prior to this case.
CASE DESCRIPTION
A 49-year-old male with no medical co-morbidities was referred to our department for evaluation of a right MCA aneurysm and an AVF. He suffered a motor vehicle accident 31 years prior, with head trauma which required extended hospitalization and multiple craniofacial surgeries, the details of which were unknown. He made a complete recovery except for residual right facial weakness. He currently presented to an external facility solely for consultation regarding facial reconstructive surgery. Magnetic resonance imaging (MRI) of the brain was performed as part of the evaluation and he was subsequently referred. Neurological review of symptoms was negative for headache, seizure, tinnitus or focal neurological deficits. On examination, he demonstrated lower motor neuron right facial paresis without any other deficit.
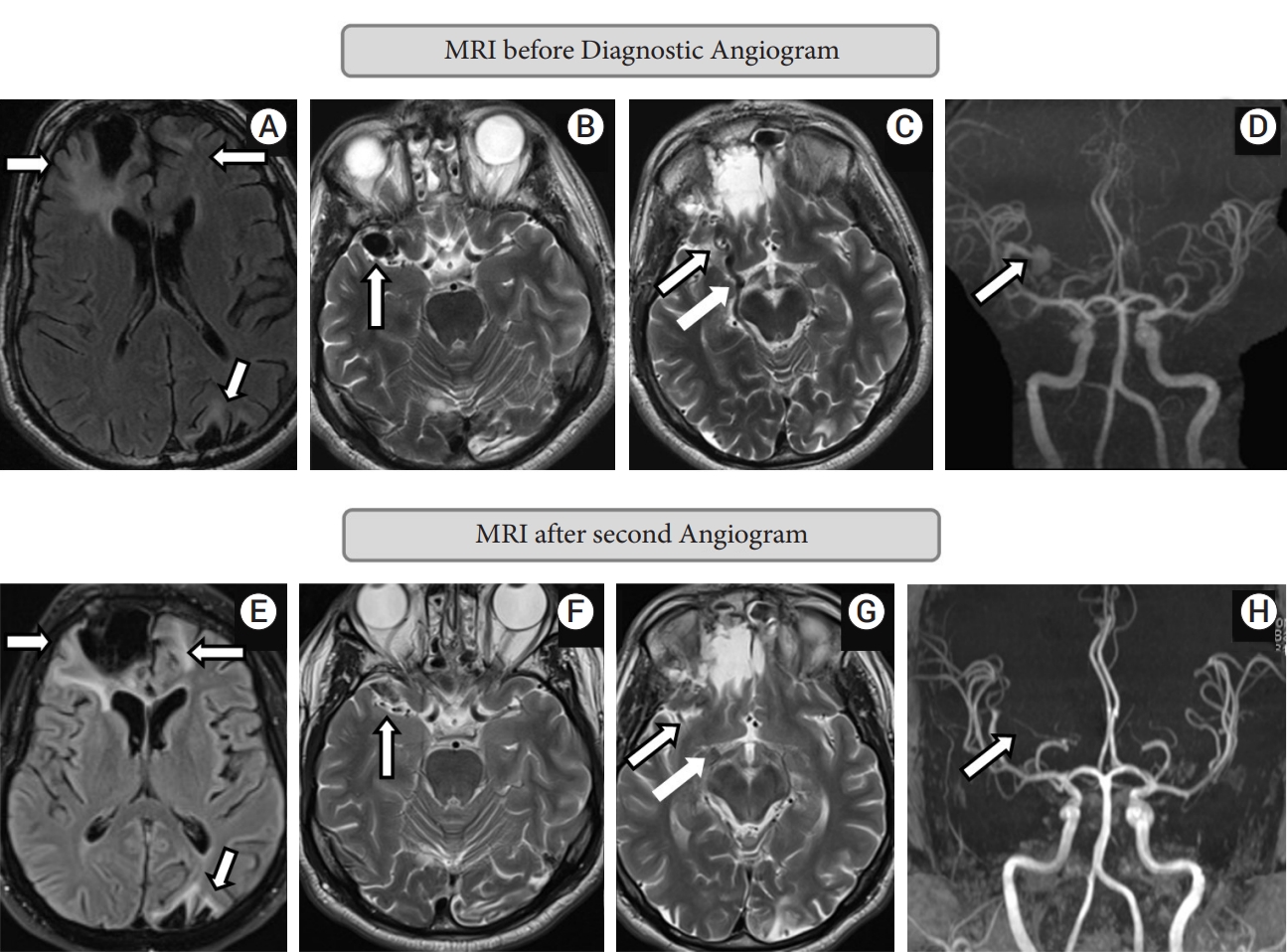
Non-contrast MRI brain showed postoperative changes of right frontal craniotomy and sequelae of prior head trauma including gliosis maximum in the right frontal lobe, but also present in the left frontal and left parieto-occipital lobes (Fig. 1A). Multiple flow voids were seen in the right middle cranial fossa, along the right MCA past the bifurcation and an enlarged right BVR was also noted (Fig. 1B, C). No obvious tangle of vessels suggestive of a nidus was seen. A non-contrast time-of-flight MR angiogram showed a frontal MCA branch aneurysm shunting into a venous varix continuing into the BVR (Fig. 1D).
Findings were suspicious for an arteriovenous fistula, and the patient was subjected to a catheter digital subtraction angiography (DSA) using Omnipaque, to completely define the angioarchitecture of the vascular malformation. OmnipaqueŌōć 300 (GE Healthcare, CO/Cork, Ireland) is a low osmolar, non-ionic contrast medium containing 647 mg of the active substance Iohexol per milliliter.
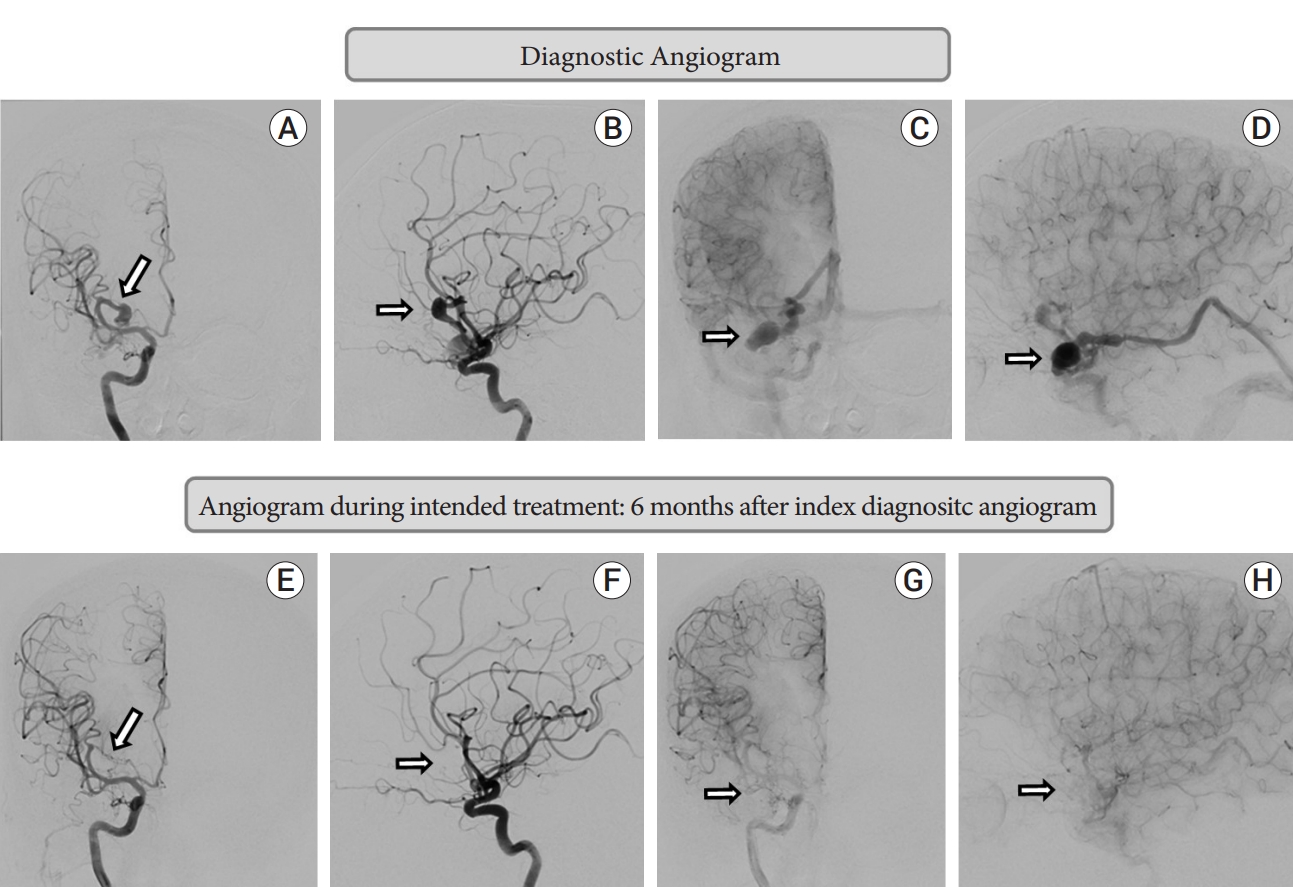
This demonstrated a complex right middle cranial fossa AVF with the predominant component being a pial fistula from a single right orbitofrontal MCA branch with direct shunting in to the BVR which harboured a venous varix at the origin, and ectatic segments. A fusiform aneurysm of the orbitofrontal feeder measuring 11 mm in largest diameter was present. There was a minor dural component with the petrous branch of middle meningeal artery shunting to the same venous varix at the origin of the right BVR (Fig. 2A-D).
Given young age, presence of a large pial shunt with the deep venous system, and associated feeding artery aneurysm, treatment with endovascular embolization was advised to mitigate the risk of future intracerebral hemorrhage. Plan was for transarterial balloon assisted liquid embolic embolization to occlude both the aneurysm and the fistulous connection, with transvenous access as backup if above not completely achieved from the transarterial route. Patient agreed for treatment but requested a delayed date.
He presented 5 months and 22 days from initial DSA for treatment. Baseline angiography showed spontaneous complete occlusion of the pial AVF, and the feeding artery orbitofrontal aneurysm (Fig. 2E-H). The minor dural supply from the middle meningeal artery had also ceased. The patient denied any interval neurological symptoms and his examination was stable. He also denied any new interval events, medications, or alternate treatments.
The patient continued to remain clinically stable thereafter. Three-month follow-up non-contrast MRI brain (Fig. 1E-G) and MR angiogram with contrast (Fig. 1H) showed no new parenchymal changes and stable complete occlusion of the aneurysm and the AVF. One-year follow-up diagnostic angiogram showed stable occlusion of aneurysm and arteriovenous fistula.
DISCUSSION
Nongalenic PAVF is a rare vascular malformation (less than 2% of all intracranial vascular malformations) in which one or more pial arteries feeds directly into a cortical vein without any intervening nidus [3]. PAVF is distinct from dural arteriovenous fistula (DAVF). In PAVF, there is abnormal direct communication or shunting between pial arteries that would normally supply the brain tissue, whereas in DAVF, vessels that normally would not supply the brain tissue are involved. On both pathologies, they feed into veins that normally drain the brain tissue. On most occasions, PAVF consists of one or more arterial feeders and usually a single venous channel. The direct arteriovenous shunt results in high venous blood flow and varix formation with the subsequent risk of haemorrhage [7]. On rare occasions, DAVF and PAVF can exist together. While the exact reasons remain unknown, PAVF can be congenital or result from iatrogenic or traumatic injury [4]. PAVF can rarely present without symptoms, but mostly present with wide range of neurological symptoms including potentially catastrophic to fatal events secondary to rupture causing intracranial hemorrhage. Considering high morbidity and mortality secondary to rupture, fistula disconnection using either microsurgery or endovascular embolization is generally advised over observation.
Spontaneous occlusion of a PAVF is an extremely rare phenomenon. The occurrence of spontaneous occlusion may be higher than DAVF, as PAVF is associated with high venous blood flow. The present case highlights the spontaneous occlusion of a large PAVF after a diagnostic DSA. Given the history of head trauma 3 decades prior, with imaging evidence of trauma sequalae, it is likely that the PAVF developed after and secondary to the traumatic event. Although we cannot be sure, it is also likely that development of the AVF was not acute since he was completely asymptomatic, suggesting a chronic pathology, possibly years. Against this background, the only modifying factor from initial diagnosis to follow-up angiography demonstrating spontaneous occlusion was the administration of intra-arterial iodinated contrast media (CM). We postulate that the iodinated CM induced thrombosis of the fistula, and explore potential mechanisms for the same.
Similar to our case, only 4 earlier cases have described spontaneous occlusion of unruptured PAVF after diagnostic cerebral angiography. Santosh et al. described spontaneous occlusion of a PAVF documented on follow-up DSA 10 days after initial angiography [11]. Satow et al. described 2 cases where spontaneous PAVF occlusion was documented on follow-up DSA 17 and 11 days after initial angiography respectively [12]. In the above 3 cases, likely initiation of thrombosis was marked by clear clinical change including new severe headache, cessation of headache, or cessation of tinnitus occurring 7 days, immediately after, and 2 days after initial angiography respectively. In our case, patient was initially asymptomatic and did not report any new or acute symptoms, suggesting slow, progressive thrombosis. In a case series of 15 patients with PAVF, a single patient showed spontaneous occlusion of a PAVF on 4-month follow-up DSA after initial angiography [7]. The report does not suggest any change of clinical features during this period. Other reports of spontaneous PAVF occlusion occurred in relation to prior surgical/endovascular interventions [5,8] or after PAVF rupture [6].
Plausible explanation for PAVF occlusion discussed in above cases is the use of intra-arterial iodinated CM. Insights into possible pathophysiological mechanisms of this phenomenon may be gleaned from reviewing the problem of iodinated CM induced acute kidney injury (CI-AKI) after vascular angiography or intervention. Vasculopathy with functionally impaired endothelial cells is a hallmark of CI-AKI [13]. CM increases the production of reactive oxygen species, the expression of vascular cell adhesion molecule-1, and the secretion of inflammatory factors (MCP-1, TNF-alpha, and IL-6) in endothelial cells [1,10]. CM also inhibit vasodilator (Nitric Oxide and Prostacyclin) production and promote vasoconstrictor (Endothelin-1) generation in endothelial cells contributing to vasoconstrictor response in renal microcirculation [2,15]. After CM injection in rats, the plasma levels of endothelial cell markers (plasminogen activator inhibitor-1 and von Willebrand factor) significantly increase [9].
Furthermore, CM also induce the release of circulating endothelial microparticles in patients with cardiovascular disease after angiography [14]. This constellation of above factors contributes to endothelial toxicity and results in its impaired role in maintaining vascular homeostasis including vascular inflammation, vascular tone and thrombosis.
We clearly acknowledge the limitation of postulating the role of iodinated CM in inducing spontaneous occlusion of unruptured PAVFs, when drawing conclusion from a single case. Almost all PAVFs undergo preoperative diagnostic DSA, and it is unclear why only a small fraction should spontaneously occlude. It is difficult to comment on the timing of such occlusion in absence of any clinical symptoms. The role of other factors including baseline comorbidities, concurrent hypercoagulable state, angioarchitecture of the PAVF or drainage patterns are unknown.
Spontaneous occlusion is certainly a rarity and canŌĆÖt be predicted. But interventionist/surgeon may be pleasantly surprised when it happens. A prior knowledge of this fact can be helpful during the intervention.
CONCLUSIONS
PAVFs are rare vascular malformations with unknown natural history, but often associated with high morbidity and mortality. Spontaneous occlusion of a PAVF is an exquisitely rare phenomenon, but can occur after cerebral angiography. This may be related to the use of iodinated CM inducing thrombosis. CM related endothelial injury could be a potential pathophysiological mechanism for the phenomenon of PAVF spontaneous occlusion.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






